Top Neurologist: Hearing Loss Causes Dementia. This I How To Ensure That Doesn't Happen
For 22 years I treated hearing loss and brain disease as separate problems. Then a Johns Hopkins researcher showed me a brain scan — and I realized how wrong I’d been. What I learned in that conference room is why I’m writing this now.

I am a neurologist.
I have spent 22 years studying the aging brain.
I have sat across from hundreds of families and explained, as gently as I know how, what dementia is going to take from them.
And for most of those 22 years, I did something I now consider a professional failure.
I treated my patients’ hearing loss and their brain health as two completely separate problems.
Hearing loss? That goes to audiology.
Memory concerns? That stays with me.
I had no idea those two things were connected.
I had no idea that the hearing loss my patients were quietly managing — telling themselves it wasn’t bad enough to do something about — was accelerating the very cognitive decline I was trying to slow.
I had no idea.
And here is what makes that harder to live with:
My own mother had untreated hearing loss for years before she developed dementia.
She was diagnosed at 77.
By 79, she didn’t recognize my face.
I am a neurologist and I never made the connection until after she was gone.
Her Name Was Dorothy. She Taught Fourth Grade for 40 Years.
My mother was sharp.
She read two books a month. She remembered the name of every student she’d ever taught. She called each of my four kids on their birthdays without looking at a calendar.
When she was 74, I started noticing she seemed a little distant.
A little slower to track conversations.
She’d ask me to repeat things.
She’d go quiet at dinner — and Dorothy Rhoads did not go quiet at dinner.
I told myself it was age.
She was managing fine.
She wasn’t having any major problems — just managing.
That phrase is the most expensive sentence in cognitive medicine.
“I’m managing fine.”
By the time she was 77, she couldn’t manage at all.
I replayed every visit, every phone call, looking for the thing I missed.
What I eventually found — years later, in a conference room in Baltimore — changed the way I practice medicine.
I Was in the Third Row When the Slide Went Up

In 2019, I attended a neurology conference in Baltimore.
I almost didn’t go. It was a crowded week.
On the second day, a Johns Hopkins researcher named Dr. Frank Lin took the stage.
He was presenting preliminary data from a trial called ACHIEVE — the Aging and Cognitive Health Evaluation in Elders trial.
I was in the third row.
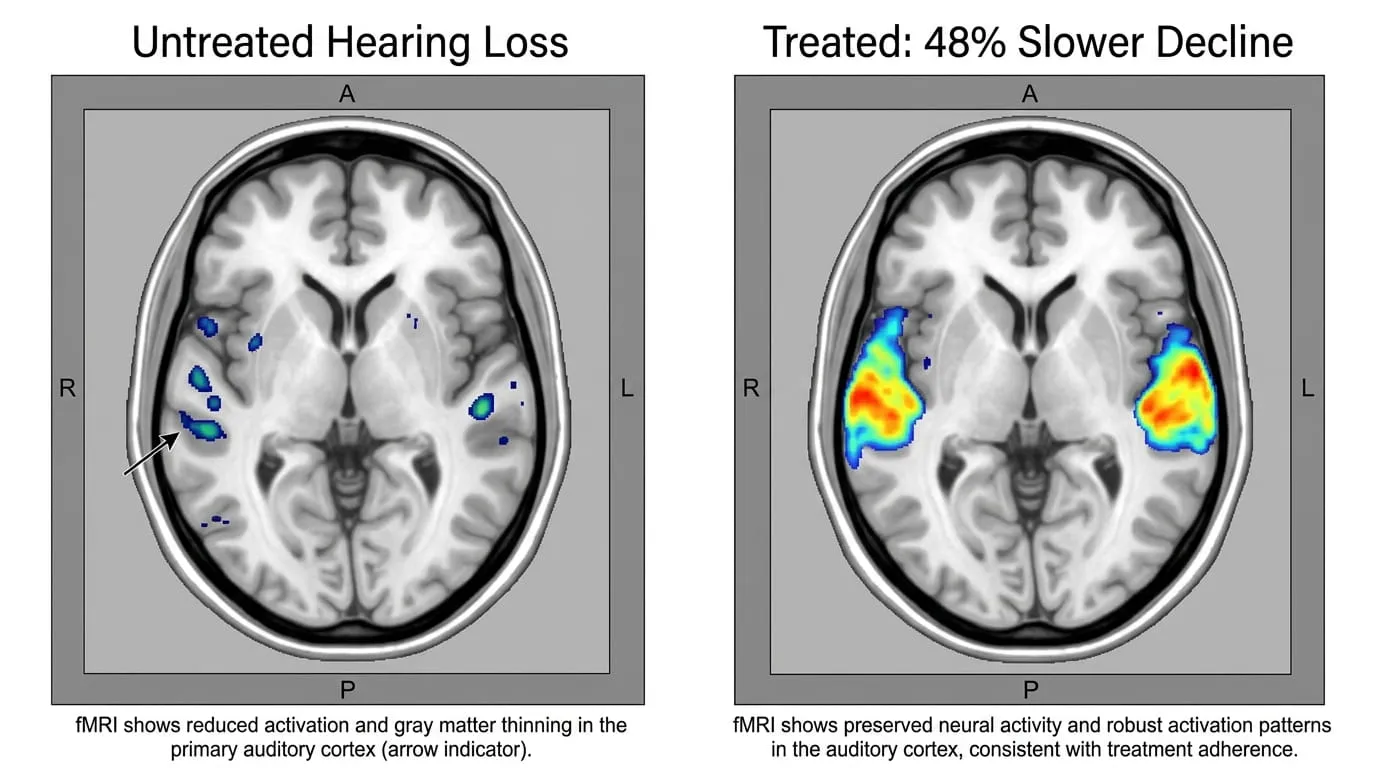
He put a slide on the screen.
It showed two brain scans side by side.
One from a patient who had treated their hearing loss.
One from a patient who had not.
The untreated brain showed measurable shrinkage — gray matter loss — in the regions responsible for memory and attention.
The treated brain did not.
I stared at that slide for a long time.
After the session, I walked up and introduced myself.
I asked him what he thought the mechanism was — what exactly was happening in the brain when hearing went untreated.
“We’ve been treating the wrong end of the problem for decades.”
That line did not leave me for weeks.
It has not left me since.
Here Is What Is Actually Happening Inside Your Brain Right Now
The problem is not simply that you’re getting older.
Every brain ages. That part is unavoidable.
The problem is what untreated hearing loss does to your brainwhile you wait.
Every time you strain to follow a conversation — at a table, in a car, on a phone call — your brain diverts resources to the task of decoding degraded sound.
Researchers call thiscognitive load.
When sound coming into the brain is unclear, the brain works overtime just to understand speech.
It pulls bandwidth away from other processes. Memory consolidation. Executive function. Attention.
This is not a metaphor. It is measurable.
And it compounds.
Do it for a year and the effect is subtle.
Do it for five years — or seven, or ten, which is how long the average person waits before treating their hearing loss — and the effect is not subtle at all.
Brain imaging studies show measurable shrinkage in the auditory cortex of people with long-term untreated hearing loss.
The brain, like any system working past its limits, begins to wear down in ways that extend far beyond the original problem.
There is also the isolation effect.
People with untreated hearing loss stop going to dinner.
They stop calling family.
They nod along in conversations they can’t fully follow.
Social withdrawal is one of the most powerful accelerants of cognitive decline known to medicine.
The two risks — cognitive load and social isolation — stack on top of each other.
The result:
It accounts for approximately 8% of all dementia cases globally.
That is more than physical inactivity. More than smoking. More than obesity.
Among people already diagnosed with Alzheimer’s disease, roughly80% have measurable hearing loss.
This is not coincidence.
This is a mechanism.
And for most people —48 million Americans have meaningful hearing loss, and only 7% are treating it— this mechanism is running unchecked right now.
I Looked at Every Option. Here Is What I Found.
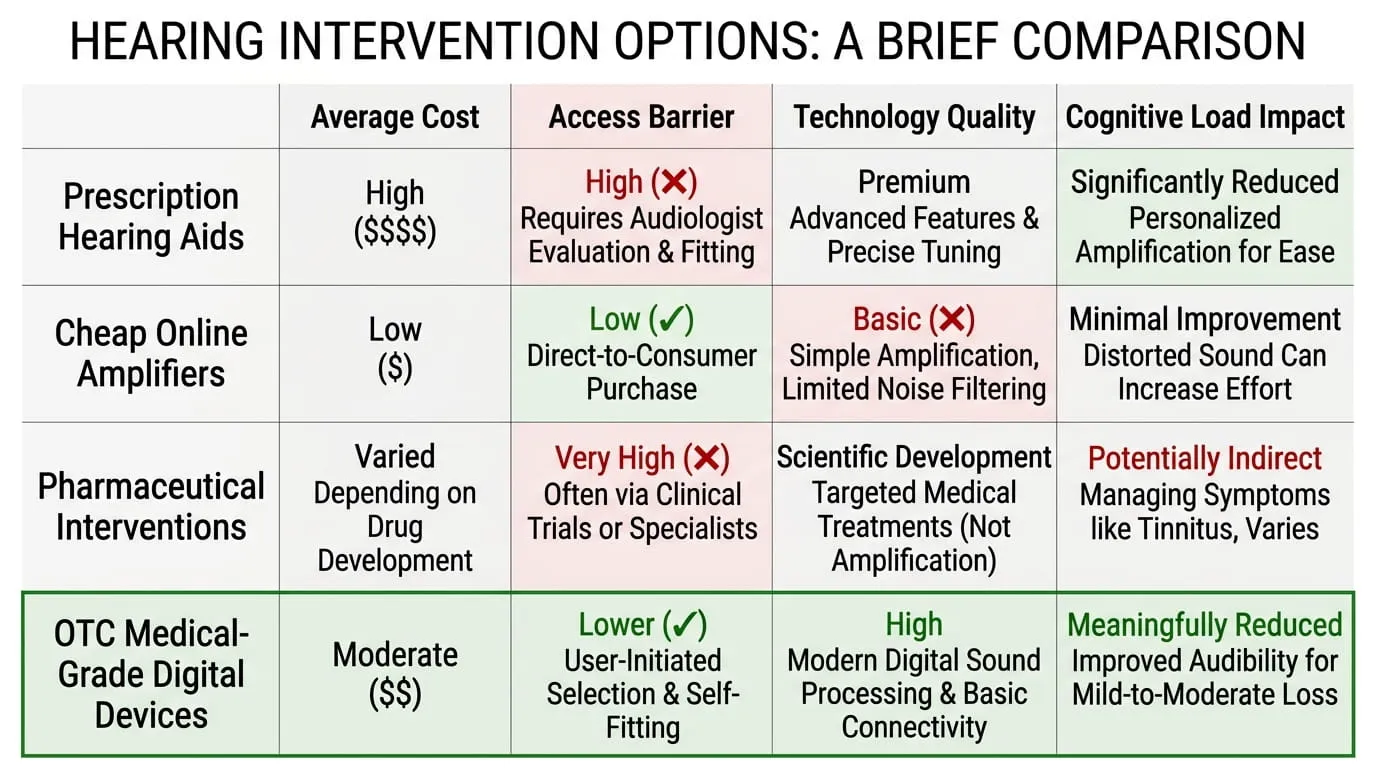
When I started taking this seriously, I looked at every available option for my patients who needed help but weren’t getting it.
The right clinical answer for many people.
The problem: the average pair costs$3,432.
Medicare does not cover them.
Getting fitted requires multiple audiologist appointments.
The process takes weeks.
For the 93% of people who need hearing support but can’t spend $3,400, this option doesn’t exist in any practical sense.
I have looked at these closely.
They are volume boosters — not hearing devices.
They amplify everything indiscriminately.
They are not calibrated to speech frequencies.
In some cases, the distorted sound they produce actuallyincreasescognitive strain rather than reducing it.
Do not confuse these with legitimate hearing technology.
There is no FDA-approved drug that treats hearing loss.
There is no FDA-approved drug that reverses dementia.
Anyone suggesting medication as the solution here is pointing you at a wall.
In October 2022, the FDA created a new product category: over-the-counter hearing aids.
For the first time, adults with mild to moderate hearing loss can access real digital hearing technology without a prescription or audiologist.
This is the category the ACHIEVE trial’s findings point toward.
Not louder.Cleaner.
Calibrated, multi-channel digital processing that gives the brain clear, accurate sound — and removes the cognitive strain that has been quietly compounding for years.
What the ACHIEVE Trial Was Actually Measuring
I want to be precise here, because this is where most reporting on this topic gets it wrong.
The Johns Hopkins ACHIEVE trial was not measuring whether hearing aids helped people hear better.
Everyone assumed they would.
The trial was measuring something far more significant.
It was measuring what happened to the brain when the strain was removed.
For three years, researchers tracked two groups of high-risk older adults.
One group received hearing intervention.
One group received general wellness counseling.
At the end of three years, the group that treated their hearing loss showed48% slower cognitive declinethan the group that did not.
Not 5%. Not 12%.Forty-eight percent.
The mechanism is what I described above — cognitive load reduction.
When the brain receives clean, frequency-accurate sound, it stops burning resources to compensate for degraded input.
Those resources become available again for memory, for attention, for reasoning.
The brain does not need to be loud. It needs to beclear.
That is what calibrated digital processing delivers.
And the data shows what happens when it does.
The Device I Now Recommend to My Patients

After the ACHIEVE data was published inThe Lancetin 2023, I started looking for an OTC option I could recommend in good conscience.
The clinical alternative — $3,400 prescription devices — was not realistic for most of my patients.
I needed something with genuine digital processing, not a volume booster.
Something with speech-frequency calibration.
Something people would actually wear every day, not leave in a drawer.
I found AmpliHear.
Here is what it has:
- Multi-channel digital processing that separates speech from background noise with real precision.
- A directional microphone that tracks the sounds in front of you — the person across the table, the TV, the phone call.
- Advanced feedback suppression that eliminates the whistling that made older hearing devices unwearable.
- Up to40 dB amplificationacross a200 Hz–8 kHz frequency response— the range that covers human speech.
- Six silicone ear tip sizes for a stable, comfortable, all-day fit.
- 20-hour battery lifeon a single charge. USB-C charging. Portable charging case.
- Nearly invisible when worn.
- Ships in 2-3 days. Ready to wear out of the box.
- No prescription. No audiologist. No fitting appointments.
The price is$99.
The cognitive protection mechanism is the same.
In independent user surveys:
- 97%of users say they would recommend it.
- 91%report improvement in group conversations.
- 86%say they can now follow TV at normal volume without straining.
I have recommended it to dozens of patients.
I have watched people who had been quietly withdrawing from conversations start showing up again.
That is not a coincidence either.
Free shipping · Ships in 2–3 days · 90-day money-back guarantee
What My Patients Are Saying
I’d been putting off doing anything about my hearing for about six years. My wife had been on me about it but I kept saying it wasn’t bad enough. My doctor told me about the Hopkins research and I finally looked into it. I was skeptical about something this affordable being worth anything — every other option I’d seen was $2,000 or more. AmpliHear showed up in three days and I put them in that evening at dinner. By the end of the meal my wife was crying. She said it was the first time in years I hadn’t asked her to repeat herself once. These are the real thing. Don’t let the price fool you.
My hearing wasn’t ‘bad’ — I’d been telling myself that for years. I could follow most conversations. I just had to work at it a little. When I read that the working at it part was the problem — that the brain strain was the actual risk — I decided to stop waiting. The difference from day one was bigger than I expected. I hadn’t realized how much effort I was putting in just to follow a normal dinner table conversation. Now I’m not putting in any effort. It just comes in clear. I ordered a second pair for my brother last month.
I’d been concerned about my memory and brought it up with my doctor. He explained the hearing-dementia connection and suggested I look at AmpliHear before we went further down the workup path. I was doubtful that something I ordered online for under $100 would be worth taking seriously. I was wrong. I’ve been wearing them for four months. My husband says I’m more present in conversations — less distracted, less frustrated. I feel it too. The 90-day guarantee made the decision easy. I kept them after the first week.
Before You Order — Read This
AmpliHear is currently available at50% offthe regular list price.
At $99 per unit, it is the most accessible entry point to the cognitive protection the ACHIEVE trial documented.
Stock at this price is not unlimited.
When demand spikes — and it does, every time this research makes the news — units sell through and shipping times extend.
If you’re reading this and the order page is still live, that means units are available now.
A quick note on cheap amplifiers being sold online.
I said this above but I’ll say it plainly:
A volume booster is not a hearing device.
Undifferentiated amplification distorts speech frequencies. It does not reduce cognitive load. It may increase it.
The mechanism that protects the brain is clean, calibrated, speech-frequency-accurate sound — not more noise.
AmpliHear is built around that distinction. Most products at similar price points are not.
The math on price:
The technology delivering cognitive load reduction in the ACHIEVE trial was not a $3,400 device.
It was calibrated digital processing applied consistently.
That is what AmpliHear delivers.
Free shipping · 90-day money-back guarantee · No prescription required
The 90-Day Guarantee
This is simple.
If AmpliHear doesn’t work for you — 29 minutes after you open the box or 29 days after you’ve been wearing it — return it.
Full refund. No questions asked.
You have 90 days from the date of purchase.
The company ships free. They process returns without hassle.
There is no financial risk to trying this.
The only risk is the one that continues if you don’t.
90 days to try it · Full refund if you’re not satisfied
How to Order

No setup. No software. No appointments.
Why most people order two units:
Hearing loss rarely affects only one ear.
The cognitive load mechanism operates on both sides — one calibrated ear and one untreated ear still leaves half the input degraded.
Most people who try AmpliHear in one ear order the second unit within a week.
Ordering two at once is more cost-effective and means you don’t lose a week of bilateral protection.
There’s also a second reason people order two:
A spouse.
If you are reading this because you’re concerned about your own hearing, there is a statistically high likelihood that the person you share a home with has the same problem.
The average person waits 7 to 10 years before treating their hearing loss.
If your spouse is in that window, they are in the same cognitive risk as you were.
Ordering two means both of you are protected.
Ships in 2–3 days · Available at getamplihear.com
Hearing Loss Doesn’t Wait. Neither Does What It’s Doing to Your Brain.
Hearing loss does not stay the same.
It progresses.
And while it progresses, the cognitive load compounds.
The gray matter continues to thin.
The connections between brain regions continue to weaken.
The social withdrawal — the quiet exit from conversations that are too hard to follow — continues to accumulate.
None of this reverses easily.
The ACHIEVE trial did not find that treating hearing lossreverseddecline.
It found that itslowedit — and that the benefit was greatest in people who acted before significant impairment had set in.
The 7-to-10-year wait is not neutral.
Every year in that window is a year of compounding.
My mother waited.
I didn’t understand what that meant until it was too late to matter for her.
I understand it now.
I cannot give her back.
What I can do is make sure the people reading this understand what she — and I — did not.
The window is open longest for people who act early.
The Conversation You’ll Have — and the One You Want to Avoid
There are two conversations ahead of you.
One is the dinner table six weeks from now — where you can follow everything, where you stop asking people to repeat themselves, where the effort is gone and you’re justpresent.
The other is the appointment, years from now, where someone hands you a diagnosis and you try to remember when you first started to notice.
I have sat across from families in that second conversation more times than I can count.
I know what it takes from people.
I know what it takes from the person in the chair.
The first conversation — the one where you just show up and hear clearly and stay in the room — costs $99 and ships in three days.
That is not a small thing.
That is the whole thing.
Act now. The cost of waiting is not measured in dollars.
Available at getamplihear.com · Free shipping · 90-day money-back guarantee · No prescription required
— Dr. James Rhoads, Neurologist, 22 years in cognitive aging
Available at getamplihear.com · Free shipping · 90-day money-back guarantee · No prescription required