Top Trichologist: Why I Stopped Telling My GLP-1 Patients Their Hair Would Come Back On Its Own — And What I Recommend Instead

Hi, my name is Dr. Sarah Maddox and I hold a PhD in Hair Biology from the University of Queensland. I've been in clinical trichology practice for 17 years and have treated over 4,000 patients with hair loss of every cause, pattern, and severity.
In the last 18 months, something changed in my clinic.
The same presentation started showing up again and again — in men and women, in people in their late twenties, their forties, their sixties. Different ages. Different backgrounds. But one thing in common.
They were on a GLP-1.
Ozempic. Wegovy. Mounjaro. Rybelsus. The drugs that have reshaped how doctors talk about weight management and metabolic disease, and that are now prescribed to tens of millions of people globally.
What they have in common — beyond weight loss — is the hair.
Here is what I see when these patients sit down across from me:
- Diffuse shedding across the entire scalp, not patches. Handfuls in the morning shower. The drain filled before they've rinsed the conditioner out. Pillowcases that look alarming in the morning light.
- The hairline thinning at the temples until the skin shows through.
- The part — once a fine white line — now wide enough that they've stopped parting their hair at all and are wearing it pulled back to hide what's underneath.
- The ponytail that is now half the circumference it was six months ago. The hair tie that goes around twice where it used to go around once.
- The hairdresser who goes quiet during the appointment. The stylist who says "there's a lot of breakage here" and then moves on without meeting their eyes.
- The photographs they've stopped taking. The social situations they've started calculating — will there be overhead lighting, will someone be behind them, will anyone be able to see the top of their head.
- And underneath all of it: the specific guilt of knowing they chose this medication. That they made a decision they believed in, that the medication is working, that they have zero intention of stopping it — and now they are watching their hair come out in their hands and being told by their prescribing doctor that it will sort itself out.
Will it?
That's the question nobody is asking carefully enough.

What if I told you that the reason GLP-1-related hair loss is so much more serious than your prescribing doctor implies — the reason that "wait and see" is one of the most harmful pieces of advice in hair medicine right now — has nothing to do with the amount you're losing, and everything to do with what happens to the follicles while you're waiting?
It sounds counterintuitive. But it's true.
And its name is perifollicular fibrosis.
Let me explain what's actually happening.
GLP-1 receptor agonists — semaglutide, tirzepatide, and the others — produce rapid weight loss. That's what they're prescribed to do, and for most people, they do it very effectively. But the human body responds to rapid, significant weight loss the same way it responds to surgery, severe illness, or extreme caloric restriction: it interprets it as a physiological emergency. And in an emergency, it starts triaging. It shunts resources toward critical functions and away from non-essential ones.
Hair is non-essential. The body does not need hair to survive.
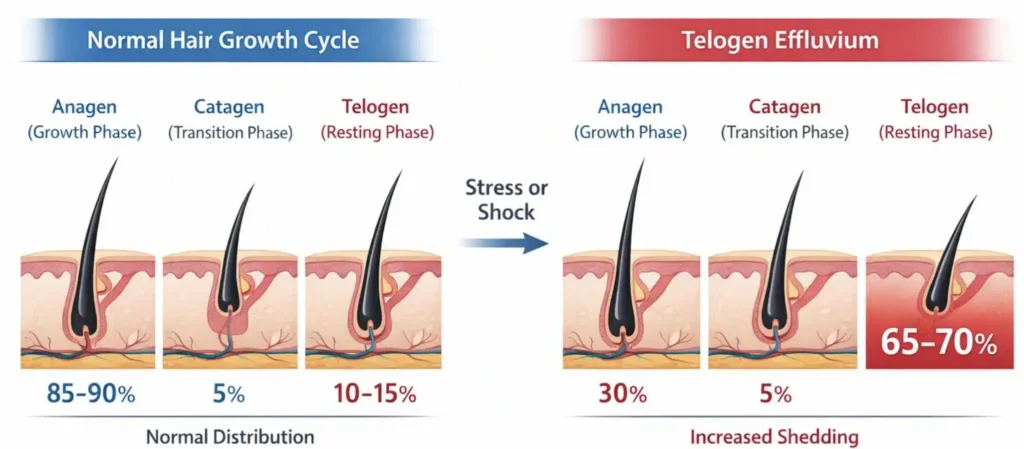
So what happens is this: follicles that are in the active growth phase — the anagen phase, when they're producing the shaft of the hair you see — are pushed prematurely into the resting phase, called telogen. They pause. They wait. They stop producing hair. And several months later — typically three to five months after the stressor began — they all shed simultaneously, because they all entered telogen at the same time.
This is called telogen effluvium. It is the mechanism behind GLP-1 hair loss. It is not mysterious. It is documented. It is caused by exactly what your medication is doing to your body.
A 2025 meta-analysis of more than 84,000 participants — peer-reviewed, published — found that people taking GLP-1 receptor agonists were 3.4 times more likely to experience hair loss than those not taking them. Not "uncommon" in the clinical trial sense. 3.4 times more likely. And in women specifically, on semaglutide specifically, the rate was more than double that seen in men.
Your prescriber may have told you this is temporary. That telogen effluvium resolves on its own within six to twelve months of onset, and that once the physiological stress stabilises, the follicles will reactivate and regrow.
That is partially true. And it is the most dangerously incomplete piece of information circulating in clinical practice right now.
Here is the part your prescriber didn't tell you.
The follicles that entered telogen are not simply paused. They are in a structurally vulnerable state.
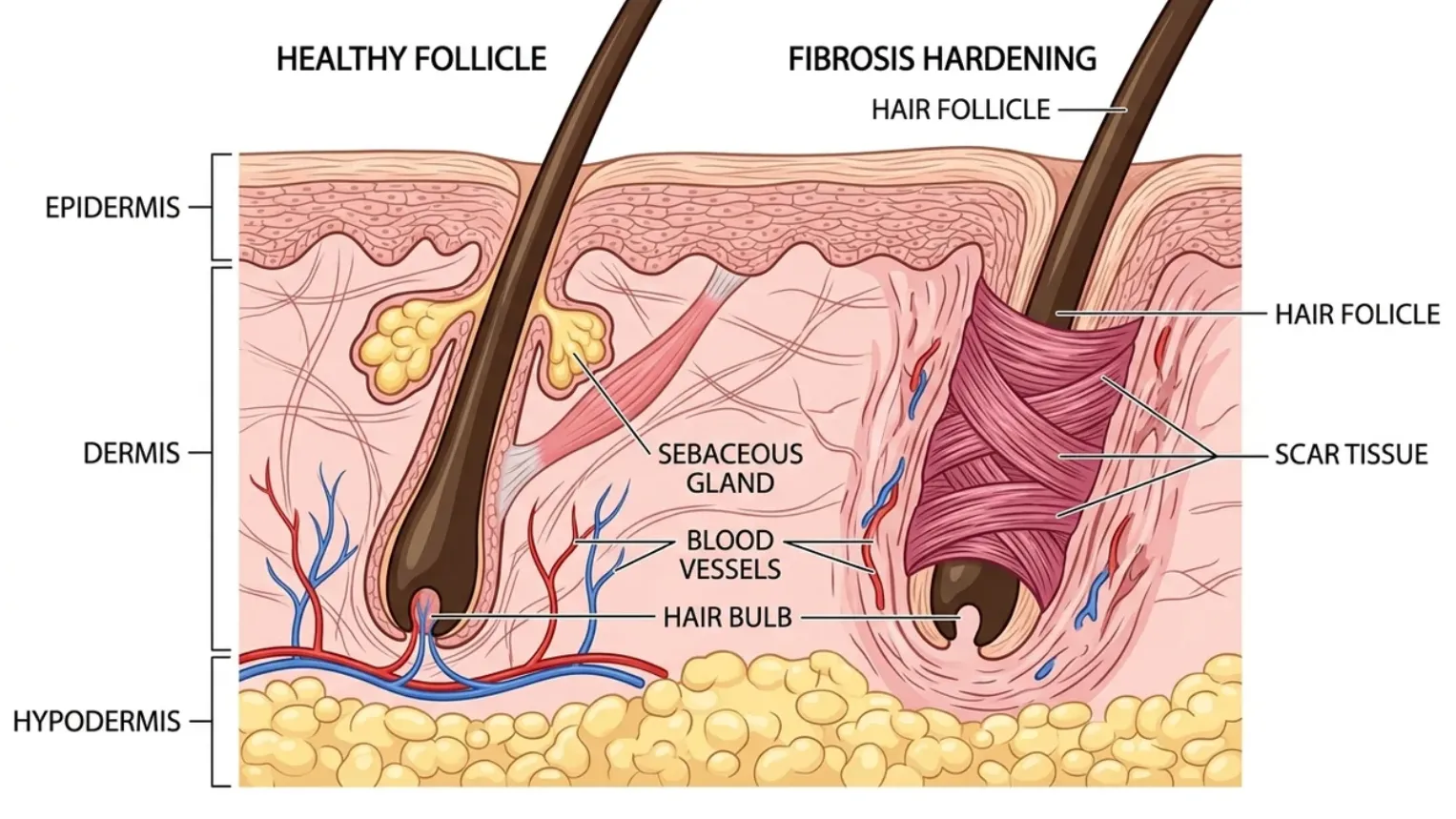
Every follicle is surrounded by a connective tissue sheath — a living envelope of collagen and ground substance that maintains the structural environment in which hair growth occurs. When a follicle is actively cycling, this sheath remains soft, flexible, and well-perfused. When a follicle enters prolonged dormancy — particularly in a body that is simultaneously nutrient-depleted from reduced caloric intake — something happens to that sheath.
It begins to stiffen.
The collagen fibres cross-link. The tissue compresses around the follicle. Blood flow decreases. The structural environment that allows regrowth progressively degrades.
This process has a specific name: perifollicular fibrosis.
It is not sudden. It is progressive. It begins during the dormancy period — not after regrowth fails. And once it advances past a certain threshold, the follicle cannot recover regardless of what you apply to the scalp afterward.
This is the clinical window. This is what "wait and see" misses completely.
When your GP says "most people's hair comes back after stopping the shedding," what they mean is: most follicles that haven't undergone significant fibrosis will eventually reactivate. What they don't say — because most prescribers have not spent time in hair biology literature — is that the fibrosis determining whether regrowth is possible is developing right now, while you're waiting.
The window to prevent permanent loss is not after the shedding stops.
It is now, during the dormancy.
Because the standard of care for telogen effluvium — in every cause, not just GLP-1 — is observation and reassurance. It's the clinical default. It requires no prescription, no specialist referral, no additional monitoring. It's what the patient information leaflets say. It's what the bulk-billing GP appointment is structured to produce.
What it is not designed to produce is a conversation about perifollicular fibrosis, the structural vulnerability window, and the topical actives that have been demonstrated to prevent it.
That conversation takes more than a standard appointment. It requires trichology training that most prescribers don't have. And the actives that address it — specifically, the anti-fibrotic compounds developed in dermatological research labs — have no pharmaceutical company lobby funding their education.
I know this because I was part of the problem.
I have a PhD in hair biology. I have been seeing patients with hormonally-driven hair loss for 17 years. I understand telogen effluvium as well as almost anyone in Australia.
And for the first four GLP-1 patients who came to me with this presentation, I told them the same thing their GP had told them.
Wait. It should resolve.
It was the patient I'll call Amy who made me realise I was wrong.

Amy was 34. She'd started Wegovy eight months before she came to see me. She'd lost 23 kilograms — results she was proud of and intended to maintain. The hair loss had started at month four. Diffuse shedding, the typical GLP-1 presentation. Her GP had told her it was temporary.
She came to my clinic not because the shedding was still happening — it had actually reduced by the time I saw her — but because the regrowth wasn't coming.
I examined her scalp under trichoscopy. What I found stopped me.
The follicle density at her crown and temples was significantly lower than expected for a 34-year-old. The follicles that should have been reactivating — entering anagen, beginning to produce new growth — were showing peripilar casts, miniaturisation, and the early structural markers of perifollicular fibrosis.
She had not been unlucky. She had been given the standard advice. She had waited the standard length of time. And while she waited, the window had begun to close.
I sent her home with the topical protocol I'll describe in a moment. After three months of consistent use, she had measurable new growth at the temples. But the crown density — the follicles that had been furthest into the fibrosis process — responded more slowly, and incompletely.
I have thought about Amy every time I've seen a new GLP-1 patient since.
Because what she needed wasn't reassurance that it would come back.
What she needed was someone who understood that the resolution of telogen effluvium is not automatic. That the structural environment of the follicle during dormancy determines whether regrowth is possible. And that addressing that structural environment requires specific topical actives — not oral supplements, not shampoos, not waiting.
That sent me down a research path that changed how I practice.
What I discovered was that the perifollicular fibrosis problem is not unsolvable. It's just that the advice people receive — wait, take biotin, use a thickening shampoo — is not engineered to solve it. It's engineered to be easy to give in a short appointment.
There is a class of topical actives that, when combined at specific concentrations and delivered directly to the scalp, addresses the structural risk of GLP-1 hair loss at the follicle level. Not every active. Not every delivery format. A specific combination.
The first thing I needed was an anti-fibrotic.
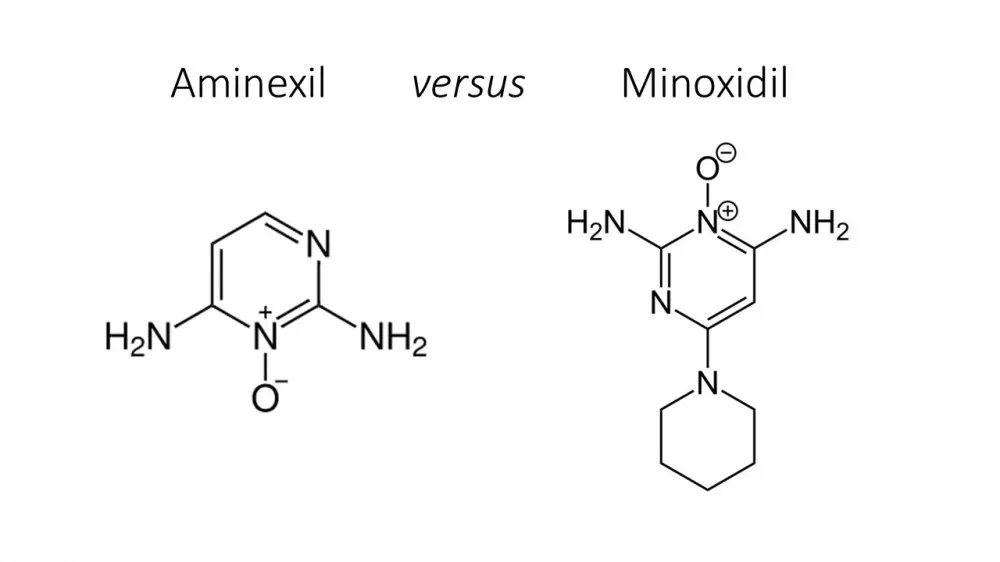
Aminexil.
Developed in L'Oréal Professionnel's clinical research laboratories. Designed specifically to inhibit the collagen cross-linking process that drives perifollicular fibrosis — the exact mechanism I was reading about. Clinical studies demonstrate that Aminexil keeps follicle tissue soft and structurally open during periods of stress, prolongs the anagen phase, anchors existing hair more securely at the root, and produces measurably fuller, stronger hair in six weeks.
Six weeks.
For a GLP-1 patient in the dormancy window, this is not cosmetic. This is the difference between a follicle that remains structurally viable for regrowth and one that doesn't.
The second piece was a DHT blocker.
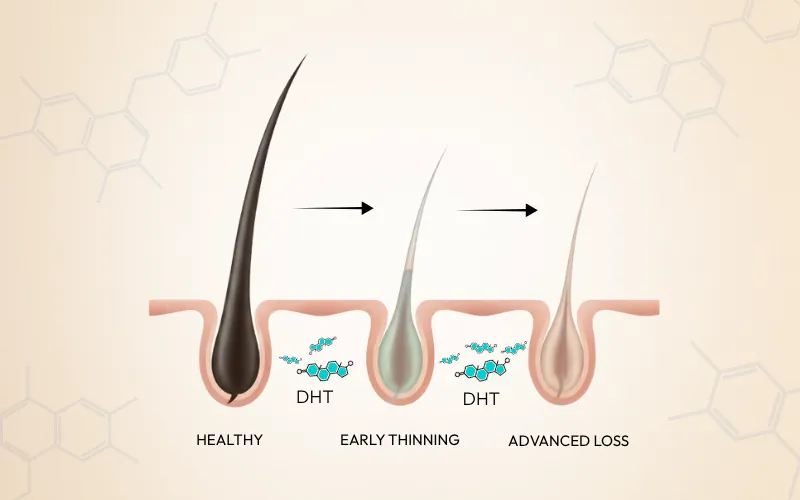
This matters because GLP-1 patients don't just have the physiological stress of rapid weight loss working against their follicles. Significant caloric restriction also shifts hormonal balance in ways that can elevate androgen activity at the scalp — compounding the follicle stress from the telogen effluvium itself. Pharmaceutical-grade caffeine, delivered topically directly to the scalp, occupies follicle DHT receptors before the hormone can bind. It independently extends the anagen phase at the cellular level — published research in theInternational Journal of Dermatologyconfirmed it penetrates the scalp within two minutes and counteracts DHT effects directly at the receptor. Not systemically. Not through the bloodstream. At the follicle.
The third piece addressed the growth cycle directly.
He Shou Wu — a botanical compound used in Traditional Chinese Medicine for over 1,300 years for age-related hair thinning. In 2020, a peer-reviewed study confirmed the mechanism: He Shou Wu elongates the anagen phase, directly abrogates androgen effects on human hair follicles in culture, and stimulates the FGF-7 gene associated with follicle regeneration. This is not anecdote. This is published mechanism. And when delivered topically at therapeutic concentration — directly to the scalp, bypassing oral metabolism entirely — it reaches the follicle at full dose.
The fourth piece is one that almost nobody talks about for GLP-1 patients specifically.
Biotin.
Not the biotin in your supplement capsule. Oral biotin, after surviving digestion, liver processing, and systemic circulation, arrives at the scalp at a fraction of the dose on the label — and most of that fraction is absorbed elsewhere. In a GLP-1 patient whose caloric intake has reduced significantly, biotin depletion is a specific documented risk. Keratin synthesis — the process that builds the hair shaft itself — depends on it.
Delivering biotin topically, directly to the scalp, bypasses every step of that dissipation. It reaches the follicle at full working concentration. It does what the capsule cannot.
Here is what I could not find anywhere: all four of these actives, in the same topical formula, at clinically meaningful concentrations. Every "hair growth" product for GLP-1 patients I found was either an oral supplement — failing the bioavailability problem entirely — or a shampoo that rinses off before anything reaches the follicle.
So I partnered with an Australian-based botanical formulation laboratory to produce the formula that didn't exist.

HaloGrow is the first topical spray I've seen that addresses GLP-1-related hair loss at the correct structural level.
Its five-active formula — anchored by Aminexil (the clinical anti-fibrotic developed in L'Oréal Professionnel's research labs), pharmaceutical-grade caffeine, He Shou Wu, topical Biotin, and Castor Oil — is delivered directly to the scalp in a once-daily spray. Nothing goes through the stomach. Nothing is processed by the liver. Everything arrives at the follicle at the concentration it takes to work.
Aminexil prevents the perifollicular fibrosis that makes temporary shedding permanent. Caffeine blocks DHT from binding to follicle receptors and extends the growth phase. He Shou Wu elongates the anagen cycle and suppresses androgen effects at the cellular level. Topical Biotin restores the keratin synthesis capacity depleted by caloric restriction. Castor Oil conditions the scalp environment and strengthens the root-to-shaft connection.
Once a day. Applied in sixty seconds along the part and at the temples. Massaged in. No rinse required. No odour. Completely absorbed.
No prescription. No pills. Nothing enters your bloodstream. No drug interactions with your GLP-1 medication. No reason to stop taking what you're taking.
But don't take my word for it.
"I've been on Wegovy for eleven months. The weight loss has been remarkable — I'm not stopping it, full stop. But at month five the shedding was genuinely frightening. I did what I always do: researched everything before I did anything. I found the meta-analysis. I found the fibrosis information. I found that biotin capsules don't reach the scalp. I was not going to spend six months on supplements that were never going to address the structural problem I'd read about. I found HaloGrow through a GLP-1 community forum where three different women had recommended it, and I looked at the ingredient list first. Aminexil, caffeine, He Shou Wu, topical biotin. I understood exactly why each one was there. That's not what a gimmick product looks like. I've been using it nine weeks. The shedding reduced noticeably by week three. I have visible baby hairs at my temples right now. My hairdresser noticed at my last appointment and asked what I was doing. I told her. She ordered her own."
"I'm a 41-year-old man on Ozempic for Type 2 management. Hair loss is not something I expected to be researching. But at month four I had a dramatic increase in shedding — my partner noticed before I was fully willing to admit it. My GP said it was telogen effluvium and told me to wait. I asked how long. He said six to twelve months. I asked what to do in the meantime. He said not much. I left that appointment and went looking. I found the fibrosis research within an hour — the piece about what happens to dormant follicles when they stay dormant too long. If the GP doesn't know about it, that's not reassuring, that's alarming. Found HaloGrow. Read the ingredient profile. Ordered the three-bottle supply that night. Twelve weeks in: shedding is down, the thinning at my crown has visibly stabilised, and I've started seeing short new growth in that area. I'm staying on my medication. My hair is not the trade-off anymore."

And I'm confident it's going to work for you too. Just imagine...
- No more standing in the shower watching what comes out and doing the mental calculation of how much is left.
- No more telling yourself it's temporary while privately not being sure it is.
- No more oral biotin capsules that are being absorbed everywhere in your body except the one place you need them.
- No more "wait and see" from a prescriber who has spent fifteen minutes on your hair biology education.
- No more positioning yourself in photos. No more scarf-covered mirrors. No more pulling your hair back to hide what's underneath.
- No more choosing between the medication that's working and the hair you had.

HaloGrow is NOT available in any pharmacy, Chemist Warehouse, salon chain, or supplement retailer.
If you see something marketed for GLP-1 hair loss in a pharmacy or on Amazon, what you're looking at is an oral supplement that cannot pass through your digestive system and reach your follicle at meaningful concentration. Or a shampoo that rinses off before it does anything. That is not the same product.
The only place you can get HaloGrow — with the full five-active formula at therapeutic topical concentration — is on the official website, where it's currently available at 70% off the regular price.
Let me give you some context on what that means.
When I first brought this formula to market, a business advisor priced it at $89 per bottle. He made a detailed case: less than one PRP session, less than two months of Viviscal, less than the supplements you've already spent money on. The logic was sound from a commercial standpoint.
But I'm not in this for the commercial standpoint. I'm in this because of Amy — and every person sitting in their GP's office being told to wait, with no understanding of what "waiting" is actually costing their follicles.
At 70% off, you're paying from $26.70 per bottle on the three-month supply.
To put that in perspective: one PRP injection session runs $1,500 to $2,500. One month of Viviscal or Nutrafol runs $80 to $130 — and does not reach your scalp. A single dermatologist appointment to discuss your hair loss runs $200 to $400 depending on your cover.
HaloGrow for a full three-month treatment course costs less than most people spend on supplements in a single month.
And because the spray maintains the scalp environment that allowed recovery to happen, most people continue using it at lower frequency after the acute phase. Prevention is easier than rescue. At this price point, keeping a bottle in the bathroom costs less than a daily vitamin.
When you see it that way, you understand what kind of offer this actually is.
But I know where you are right now. I'm not naive about it.
You started a medication that is working for the reason you started it. You didn't sign up for the hair loss. You've been told it's temporary and you've been trying to believe that, but you've also been watching the drain and doing the maths on whether "temporary" actually applies to you.
You may have already bought biotin. It may not have done much. You're wondering whether anything topical is actually going to make contact with the problem.
I hear that.
Which is why I'm not just offering HaloGrow at 70% off.

You have 30 days to use HaloGrow and watch what happens to your follicles.
Count the hairs in the drain. Photograph your part. Run your fingers along your temples and feel for the baby hairs that should be there. Look at your ponytail.
If at the end of 30 days you haven't seen the shedding reduce, the density stabilise, or the first fine hairs beginning to come through — email us. Every dollar comes back. No forms, no retention team, no store credit. Your refund processes within 48 hours.
The only thing you risk is nothing. Because if it doesn't work, you don't pay.
Click the button below — it takes you to the official HaloGrow website where your 70% discount is automatically applied.
From there, you'll see the checkout page. Enter your name, your shipping address, and your payment information. Select how many bottles you want to order.
Most people who are serious about protecting their follicles during active GLP-1 treatment order the 3-bottle supply. Here's why that matters specifically:
The window during which Aminexil can prevent perifollicular fibrosis is the period of follicle dormancy — which, for GLP-1 patients, typically spans the three-to-five months after shedding onset and up to the twelve-month mark. A 3-bottle supply gets you through the critical structural protection window without a break in daily application. No gap in coverage. No allowing fibrosis to advance during a reorder delay.
The 3-bottle supply is also where the discount goes deepest. You're protecting more of the window for less per day than a single bottle.
The 6-bottle supply is there for people who want a full year of protection plus ongoing prevention maintenance — or for anyone with a partner or family member who started a GLP-1 recently and is watching their hair change.
But even a single bottle will show you whether the fibrosis risk is being addressed. Most people know within two to three weeks. The drain tells you first.
I know what happens when you decide to keep waiting.
I've seen it in my clinic. You tell yourself the GP is probably right and it will come back. You wait month four. Month five. Month six. The shedding does reduce — because that's what telogen effluvium does, it runs its course. But the regrowth doesn't arrive the way you expected. The temples stay thin. The crown stays sparse. You go back to your GP. They say: "Some hair loss can be permanent." You ask why nobody mentioned that. They don't have a good answer.
I'm not saying that to frighten you. You've probably already felt the quiet fear under the surface of "it'll come back."
What I'm saying is that the decision you make today is not a minor one.
This isn't just about hair.
It's about staying on the medication that is working without paying a toll you weren't told about. It's about being in the photos at the milestones happening this year. It's about wearing your hair the way you wore it before the shedding started. It's about not spending the next six months hoping, then the six months after that grieving, then the rest of it adjusting.
You don't have to choose between the weight loss and the hair anymore.
A real solution exists. It addresses the structural risk at the follicle level — the perifollicular fibrosis that turns temporary shedding into permanent loss. Nothing enters your bloodstream. No drug interactions. No contraindications with your GLP-1. No prescription. No waiting.
It's on the other side of that button.
If it doesn't protect your follicles as promised, you don't pay.
Demand for HaloGrow among GLP-1 users has increased dramatically following coverage in multiple health and wellness publications. Inventory is limited. Order yours before stock runs out.