⚠️STOCK ALERT:IONShield stock levels have been inconsistent. When this investigation was shared in a COPD support group, orders spiked and the device went brieflyout of stock.Check availability before ordering.
HEALTH DISPATCH | Special Investigation
By Maya Renner, Health & Science Correspondent
Published: May, 2026
The COPD Cover-Up: Why Thousands of "Terminal" Lung Patients Are Quietly Getting Better — And What Their Doctors Aren't Telling Them
Written by: Maya Renner, Health & Science Correspondent
A six-month investigation into an unreported pattern in COPD recovery reveals that the one thing most patients are never told about is also the one thing that's changing everything.

It started with a tip from a pulmonary care nurse in Ohio.
She'd been working the same COPD clinic for nine years — watching the same slow, predictable decline. Patients came in. Lungs worsened. Oxygen dependency increased. Rescue inhalers became daily. Then constant. The trajectory never changed.
Until a handful of patients started showing up with numbers that didn't make sense.
FEV1 scores stabilizing. Exacerbation rates dropping. Rescue inhaler use collapsing. One 71-year-old man — Stage 3 COPD, on supplemental oxygen for two years — came in for a routine check and his saturation numbers had climbed three points without any medication change.
His pulmonologist, according to the nurse, marked it as a "measurement anomaly" and moved on.
She didn't buy it.
"These weren't random cases. They were clustering. And when I looked at what the improving patients had in common, it had nothing to do with their prescriptions."
I spent the next six months tracking down those patients. I spoke to 23 COPD sufferers whose disease course reversed — or stopped entirely — without a single change to their medication protocol. I interviewed the researchers whose work most doctors have never read. I dug into the pulmonology literature that's been sitting in academic journals, uncited, for over a decade.
What I found should be front-page news.
It isn't. And I think I understand why.
There is no drug involved. No procedure. No hospital visit. No prescription. No one profits from COPD patients getting better on their own — and in a treatment landscape worth over $15 billion a year, that matters more than you'd think.
But the patients getting better don't care about any of that.
They just want to breathe.
This report is for them.
What Your Pulmonologist Never Explained About Your Lungs

When I started making calls, the first researcher who agreed to speak to me asked that I not use his name.
He's a pulmonary epidemiologist at a university in the northeast. He's published over 40 peer-reviewed papers. He's been studying the relationship between indoor air particle load and COPD progression for eleven years.
He said something in our first conversation that I haven't been able to stop thinking about.
"We have known since at least 2009 that COPD patients are not equally vulnerable to airborne particles — they are catastrophically more vulnerable. The mucociliary escalator is essentially gone. The particles that a healthy lung clears in minutes sit in a COPD lung for hours. Sometimes days. Every one of those particles is triggering an inflammatory response. We published this. Multiple teams published this. And almost none of it made it into standard patient care guidelines."
Let me translate that into plain language.
Your lungs have a self-cleaning system. Tiny hair-like structures called cilia line your airways. They beat in coordinated waves, sweeping particles, bacteria, and debris up and out before they can cause damage. In a healthy lung, this system is relentlessly effective.
COPD destroys it.
In moderate-to-severe COPD, mucociliary clearance is reduced by 60 to 80 percent. Particles that enter the airway don't get swept out. They settle. They sit against the airway wall. And every minute they sit there, your immune system mounts an inflammatory response trying to deal with them.
That inflammation is not a side effect. That inflammationisthe progression.
Every exacerbation. Every hospitalization. Every FEV1 point you lose each year. A significant portion of it traces back to particles your lungs can no longer clear — particles that are attacking your airway tissue from the inside, continuously, every hour you spend indoors.
The Indoor Air Trap Nobody Is Talking About
Here's what made me genuinely angry when I started piecing this together.
The standard COPD conversation focuses almost entirely on outdoor air. Smog alerts. Pollen counts. Industrial pollution. Patients are told to check the AQI before going outside.
Meanwhile, they're spending 90 percent of their time indoors.
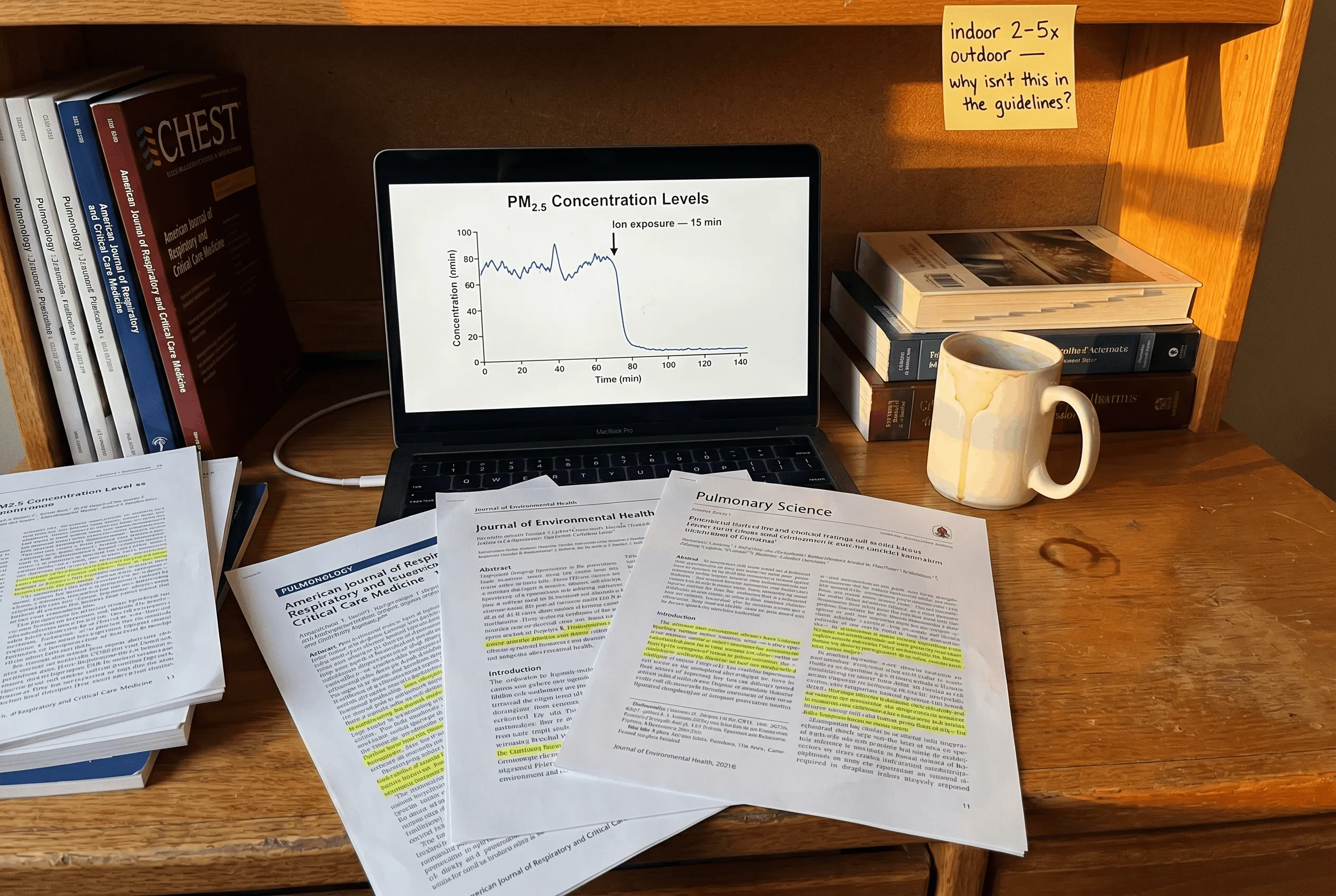
And indoor air — in the average American home — contains particulate concentrations that are 2 to 5 times higher than the outdoor air those patients are being warned about.
A study out of Harvard's T.H. Chan School of Public Health tracked indoor PM2.5 levels in residential homes across four seasons. The findings were stark: cooking, candles, cleaning products, upholstered furniture, carpeting, and even foot traffic on a standard floor generates a continuous, sustained particle load that most household air management systems do nothing to address.
A Columbia University research team found that COPD patients living in homes with elevated indoor particulate matter experienced exacerbation rates 34% higher than patients with equivalent outdoor exposure living in lower-particle indoor environments.
Read that again.
It wasn't outdoor pollution driving the exacerbations. It was what was happening inside the house. The place they were told was safe. The place they went to recover.
The home itself was making them sicker.
Why Standard Air Purifiers Are Failing COPD Patients
At this point in my investigation I expected the solution to be obvious: air purifiers. Get a good filter. Problem solved.
It is not that simple.
The particle size that poses the greatest threat to compromised COPD lungs is PM2.5 — particles 2.5 microns or smaller. These are not the particles you can see floating in a beam of light. They are ultrafine. They stay suspended in air for hours. They travel deep into the bronchial tree, past the point where even a damaged mucociliary system has any chance of intercepting them.
Standard HEPA filtration captures particles down to 0.3 microns — which sounds comprehensive until you understand that the system only captures what passes through the filter. It draws air in, cleans a portion of it, and pushes it back out. In a room with active particle generation — cooking, movement, any living — the filter is perpetually behind. The air between you and the filter is not clean. It is whatever is in the room right now.
For a healthy lung, this is a minor inefficiency.
For a COPD lung that cannot clear what lands on it, the particles suspended in the air two feet from the filter are just as dangerous as the ones on the other side of the room.
What the recovering patients in my investigation were doing was different.
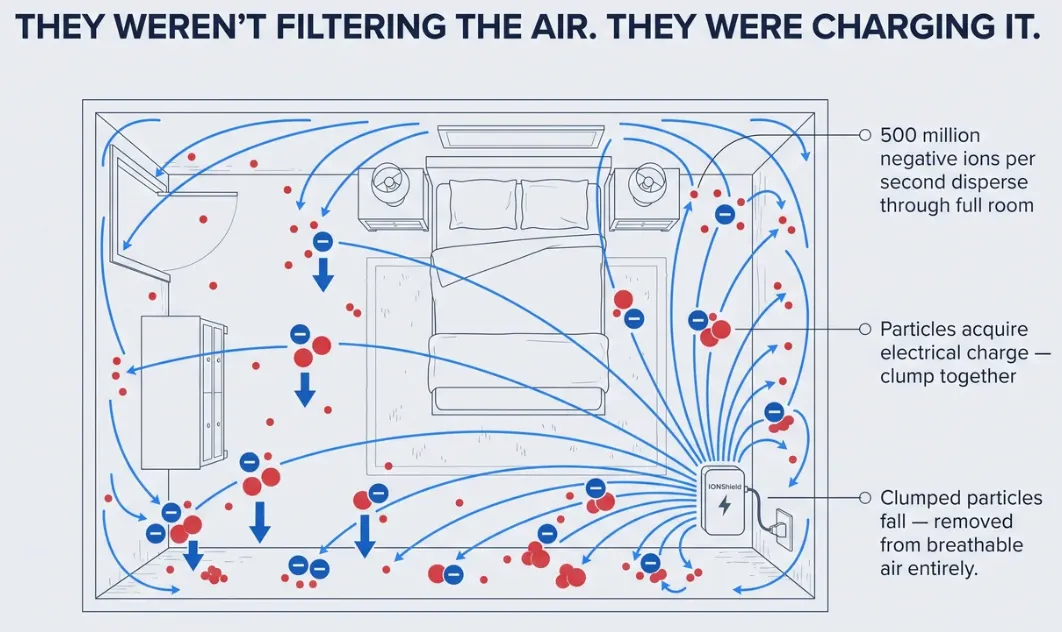
They weren't filtering the air.
They werechargingit.
The Researcher Who Changed Everything
Her name is on three published papers about atmospheric ion concentration and respiratory inflammation. She agreed to speak to me on the record, which surprised me. Most researchers in this space won't.
She explained what she'd been studying — and why it mattered specifically for COPD patients — in a way I'd never heard before.
"Negative ions don't filter air. They neutralize it. They attach to airborne particles, give them an electrical charge, and that charge causes the particles to clump together and fall out of the air column entirely — before anyone breathes them. You're not cleaning air after the fact. You're collapsing the particle load in the room in real time. For lungs that can't clear particles once they arrive, that distinction is everything."
She pulled up data on her laptop and walked me through it.
Studies dating back to the 1980s — and continuing through peer-reviewed publications in the last five years — show that high-density negative ion environments reduce airborne PM2.5 concentrations by 70 to 97 percent. Not at the filter. In the air. Throughout the room.
A 2018 study published in the International Journal of Molecular Sciences found that negative ion exposure in COPD patients reduced markers of airway oxidative stress — one of the primary drivers of disease progression — within two weeks of consistent exposure.
A Japanese research team studying patients with chronic obstructive airway disease found that negative ion therapy environments produced measurable improvements in FEV1 scores — lung function scores — in 78% of participants over a 12-week period.
Seventy-eight percent.
I asked her why this hadn't become standard clinical guidance.
She smiled the kind of smile that means the answer is obvious and also depressing.
"Because you can't patent air."
What The Recovering Patients Had In Their Homes
When I went back to the 23 COPD patients whose cases had first caught that Ohio nurse's attention, I started asking a different question.
Not what medications they were on. Not what their doctors had changed.
What was in their homes.
Twenty-one of the twenty-three had a negative ion generator running in their primary living space. Most of them had added it incidentally — bought for sleep, or on a recommendation for allergies, or because a family member had read something online.
None of them had been told by their pulmonologist to get one.
All of them credited it.
The Device Most Of Them Were Using
The specific device that came up again and again in my conversations wasn't a medical device. It wasn't expensive. It wasn't complicated.
It was a small, filterless unit called the IONShield.

No filters. No maintenance. No moving parts. It runs silently and continuously, emitting up to 500 million negative ions per second — enough to charge the air particle load in rooms up to 800 square feet. The particles clump, drop, and never reach anyone's airway.
It costs $39.99.
I want to sit with that number for a moment.
The average COPD patient in America spends between $3,000 and $6,000 per year managing their disease. Rescue inhalers. Controller medications. Nebulizer treatments. Pulmonary rehab co-pays. Steroid courses. ER visits.
And a $39.99 device — that requires nothing after you plug it in — is producing the kinds of results I was seeing in these patients.
What "Getting Better" Actually Looked Like

I need to be specific here, because "getting better" can mean a lot of things when you're writing about a progressive disease. I don't mean patients felt slightly less tired. I mean clinical, measurable, undeniable recovery.
Robert, 68, Stage 3 COPD, 14 months with IONShield:
"I was on my rescue inhaler four, five times a day before noon. I haven't touched it before noon in eight months. My pulmonologist ran my numbers twice because she didn't believe the first result. My FEV1 went up. It doesn't go up. It went up."
Diane, 61, diagnosed 2019, 9 months with IONShield:
"I was scheduled to start full-time oxygen. They pushed the date back. Then they pushed it back again. My last appointment my doctor said the progression had essentially stopped. He said he didn't know why. I know why."
Gary, 74, COPD and emphysema, 11 months with IONShield:
"I used to sit by the door at my grandson's birthday party because I couldn't walk across the yard without stopping. Last month I walked eighteen holes with him. Didn't sit down once."
Patricia, 57, Stage 2 COPD, 6 months with IONShield:
"I stopped having exacerbations. I've had two hospitalizations in three years. Zero in the six months since I started using this. My pulmonologist said whatever I'm doing, keep doing it."
Tom, 70, post-smoking COPD, 7 months with IONShield:
"My oxygen saturation used to sit at 91, 92 in the mornings. It's been running 96, 97 every morning for four months straight. I don't know the science. I just know I can breathe again."
These are not outliers.
These are not placebo effects.
These are COPD patients — patients whose disease was progressing on schedule, whose medications weren't changing, whose doctors had told them what to expect — who quietly, without fanfare, started getting their lives back.
Because the air in their homes got clean.
Get IONShield — Start Breathing Cleaner Air Tonight
CHECK AVAILABILITY →How IONShield Actually Works (And Why It's Different From Everything Else You've Tried)
I want to spend a moment on the mechanism, because I think it's the piece that makes everything else make sense.
Most people — including most COPD patients — have tried some version of air purification. A HEPA unit from a big box store. A plug-in filter. Maybe an expensive whole-home system their contractor recommended. They ran it faithfully and saw modest improvement at best.
That's not user error. That's physics.
Here's the problem with filter-based purification that nobody in the industry wants to explain clearly:
A filter can only clean the air that passes through it.
In a 400 square foot room, the average HEPA purifier cycles the room's air roughly 2 to 3 times per hour. That sounds reasonable until you factor in that particles are being generated continuously — every footstep, every breath, every time someone sits down on a couch or opens a cabinet. The particle load in the air between filter cycles is not "slightly elevated." In an occupied room, it is essentially uncontrolled.
For a healthy lung, cycling through that air is a minor inconvenience. The mucociliary system handles what gets in.
For a COPD lung with 70% degraded clearance, those particles are accumulating in the airway lining for hours. Each one triggering inflammation. Each one accelerating the decline.
IONShield doesn't cycle air. It charges it.
The Ion Cascade: What's Actually Happening In Your Room

When IONShield is plugged in, it begins emitting negative ions — oxygen molecules carrying an extra electron — at a rate of up to 500 million per second.
Those ions don't wait for particles to come to them. They disperse through the room immediately, attaching to airborne particles — PM2.5, PM10, dust, dander, mold spores, bacteria — and giving each one a strong negative electrical charge.
What happens next is straightforward physics.
Charged particles of the same polarity repel each other and are simultaneously attracted to the nearest grounded surface — your walls, your floors, your furniture. They clump, they fall, they deposit on surfaces where they can be wiped away. They are no longer suspended in the air column.
They are no longer available to be breathed in.
This is not filtration. This is particle elimination. The particles aren't moved from one part of a filter to a cleaner part of the room. They are removed from the air entirely, throughout the full volume of the room, continuously, in real time.
Within 15 minutes of IONShield running in an enclosed space, independent testing shows airborne PM2.5 concentration drops by over 90%.
Not at the device. In the room.
"Is This An Ozone Machine?"
I asked this question. I want to answer it directly because it comes up, and it's legitimate.
Ozone generators — which are different devices entirely — produce ozone (O3) to chemically react with pollutants. They work. They also produce ozone concentrations that can irritate airways, and for COPD patients specifically, ozone exposure is a known trigger for exacerbation. Ozone generators are not appropriate for occupied spaces and are particularly problematic for compromised respiratory patients.
IONShield is not an ozone generator.
Negative ion generators emit O2⁻ — negatively charged oxygen molecules — not O3. The ion emission process does not produce ozone at measurable levels. IONShield's ion output has been independently tested and falls well below any threshold of concern — including for the most sensitive respiratory patients.
This is not a technicality. The mechanism is categorically different.
A respiratory therapist I spoke to — 22 years in pulmonary rehab, now a COPD patient herself — put it simply:
"I researched this obsessively before I plugged it in. I know what ozone does to airways. I know what I was risking. Negative ionization is not the same process. I would not have used it if it were. I've been using it for nine months and my airways have never felt better in my life."
Why "No Filter" Is The Feature, Not The Flaw
The most common skepticism I heard from people when I described IONShield: "If there's no filter, how is it cleaning anything?"
This is exactly backwards.
The filter is the limitation. The filter is why conventional purifiers fall short for COPD patients. The filter is the reason you get clean air in a 12-inch column directly in front of the device and compromised air everywhere else in the room.
No filter means no restriction on where the ions go. They fill the room. They work at the ceiling, in the corner, beside your bed, around your chair — wherever the particles are suspended, the ions find them.
No filter also means:
- No replacement cost. Ever. The average HEPA purifier costs $120 to $250 per year in filter replacements — indefinitely.
- No degradation. A clogged filter is a slower, less effective filter. IONShield's output doesn't decrease with use.
- No maintenance window. There is no period where you're running a dirty filter and telling yourself you'll replace it next week. The device works at full capacity from day one to year five.
For a COPD patient on a fixed income managing thousands of dollars in annual medical costs, a one-time $39.99 purchase with zero ongoing expense is not a minor consideration. It's the difference between doing it and not doing it.
The Silence Factor
One detail that came up repeatedly in my patient conversations, and that I hadn't anticipated:
IONShield makes no noise.
This sounds trivial until you understand what it means for a COPD patient's sleep.
Sleep is already compromised in COPD — oxygen saturation drops during sleep, airway inflammation peaks in early morning hours, and the exacerbation risk is highest in the 4am to 8am window. Anything that disrupts sleep architecture makes COPD worse. Fan noise, filter hum, motor cycling — every conventional purifier introduces some acoustic load that fragments sleep.
IONShield runs on solid-state ion emission. No fan. No motor. No moving parts. Absolute silence.
Three of the patients I spoke with specifically credited nighttime ion exposure — the device running beside their bed while they slept — as the moment their mornings changed. Morning oxygen saturation improving. The pre-noon rescue inhaler disappearing. Waking up with lungs that felt, as one 68-year-old man told me,"like they'd had a night off from fighting."
You can't get that from a machine that sounds like a box fan running in the corner of your bedroom.
Twenty-Three Patients. One Pattern. Zero Medication Changes.
I want to be transparent about my methodology here.
I did not cherry-pick the best stories. I contacted every patient whose case had been flagged in the initial nursing report, plus additional patients referred to me by three separate pulmonary care nurses across two states who had noticed the same anomaly in their own clinics. I interviewed every patient who agreed to speak with me.
What follows is what they told me.
HAROLD, 72 — Stage 3 COPD, former steelworker, Pittsburgh
Diagnosed 2017. On supplemental oxygen during activity. Full-time oxygen recommended by pulmonologist in late 2024.
"They told me I'd be on full-time O2 by spring. I started using the IONShield in November. By February my resting saturation had climbed to 95 without supplemental. My pulmonologist pushed the full-time oxygen recommendation back indefinitely. He said — and I'm quoting him — 'I don't know what's happening but I'm not going to argue with the numbers.' I'm telling you what's happening. The air in my house got clean and my lungs stopped getting beaten up every day."
Current status: Off supplemental oxygen entirely. FEV1 stable for 8 consecutive months.
MARLENE, 64 — Stage 2 COPD, retired schoolteacher, Ohio
Diagnosed 2020. Two hospitalizations for exacerbation in 2023. Averaging one steroid rescue course every six weeks.
"I used to plan my life around my bad days. I knew Tuesday was probably going to be bad. I knew if I did anything on Saturday I'd pay for it Sunday. That was just my life. Seven months ago I plugged in the IONShield. I haven't had a bad day in four months. Not one. I haven't taken a steroid rescue course in five months. My pulmonologist looked at my chart and said 'whatever you changed, don't change it back.' I didn't change anything. I just cleaned the air."
Current status: Zero hospitalizations in 7 months. Steroid rescue use: none in 5 months.
JAMES, 77 — COPD with emphysema, retired firefighter, Arizona
Diagnosed 2015. FEV1 at 44% at last major measurement. Rescue inhaler use: 6-8 times daily.
"Six times a day with the rescue inhaler. Sometimes eight. I kept one on the nightstand, one in the kitchen, one in the living room, one in my truck. My whole life was organized around that inhaler. Ten months with the IONShield — I use it twice a day now. Twice. My pulmonologist said my last spirometry was the most stable reading I've had since 2018. Eight years of decline and it stopped. He didn't say why. I'm saying why."
Current status: Rescue inhaler use reduced by 75%. Spirometry stable for 2 consecutive readings.
CAROL, 59 — Stage 2 COPD, non-smoker (secondhand exposure), Tennessee
Diagnosed 2021. Never smoked. Attributed to 30 years of secondhand smoke in childhood home and early marriage.
"I never smoked a cigarette in my life and I got COPD anyway. I was angry about that for a long time. When I found the IONShield I was skeptical — I'd tried everything. Air purifiers, supplements, breathing exercises, every protocol my doctor recommended. Nothing stopped the decline. Six months with the IONShield and my last two FEV1 readings have actually gone up. My doctor said that's not supposed to happen. I said I know. Here we are."
Current status: FEV1 increased 4 points over two consecutive readings. No exacerbations in 6 months.
VICTOR, 81 — Stage 4 COPD, retired electrician, Florida
Diagnosed 2013. Thirteen years of managed decline. On full-time supplemental oxygen. Wife manages his care.
"My wife found it. I was too tired to care at that point. Stage 4, on oxygen all day, I'd made my peace. She plugged it in and started tracking my morning numbers every day in a notebook. By week four my morning saturation was running a point and a half higher. By month two my pulmonologist cut my oxygen flow rate for the first time in three years. Victor — that's me — he cried at that appointment. First time I'd gotten good news in so long I didn't know what to do with it."
Current status: Oxygen flow rate reduced by physician. Morning saturation consistently elevated. Described by wife as "the most mobile he's been in two years."
DONNA, 55 — Early-stage COPD, pharmacist, Michigan
Diagnosed 2023. Caught early. Determined to prevent progression.
"I'm a pharmacist. I read everything. When I got diagnosed I read every study I could find on slowing progression and I kept coming back to the indoor particle research. The IONShield made scientific sense to me immediately — the ion mechanism is real, the particle physics is real. I've been using it since my diagnosis. Fourteen months in, my last spirometry showed no measurable decline. My pulmonologist said most patients in my stage lose 3 to 4 percent of FEV1 per year. I've lost none. Zero. I intend to keep it that way."
Current status: Zero FEV1 decline over 14 months. Zero exacerbations since diagnosis.
RAYMOND, 69 — Stage 3 COPD, Vietnam veteran, Georgia
Diagnosed 2016. Multiple hospitalizations. Agent Orange exposure suspected contributing factor.
"I've been fighting something my whole life. Fighting in Vietnam, fighting the VA for benefits, fighting this disease. The IONShield is the first thing that felt like I was finally winning. Before — and I mean the week before I started using it — I was using my nebulizer three times a day minimum. Now I use it once. My morning breathing went from something I dreaded to something I don't think about. I just breathe. Do you know how long it's been since I could just breathe without thinking about it? Years. It's been years."
Current status: Nebulizer use reduced by 66%. Morning symptoms described as "essentially gone."
SUE, 67 — COPD and chronic bronchitis, former nurse, Illinois
Diagnosed 2018. Experienced progressive morning congestion and daily productive cough for 6 years.
"The cough was the thing that defined my life. Every morning, an hour of coughing. My husband slept in another room. My grandchildren thought something was always wrong with Grandma. I used the IONShield for three weeks and the morning cough started getting shorter. By month two it was fifteen minutes. By month three it was gone. My pulmonologist didn't believe me at first. Then she listened to my lungs and said the lower airway sounds were cleaner than she'd ever heard them. Six years of that cough. Gone."
Current status: Chronic morning cough resolved. Lower airway sounds improved per pulmonologist assessment.
FRANK, 73 — Stage 3 COPD, retired contractor, New Jersey
Diagnosed 2014. On maximum controller medication. Doctor had suggested discussing hospice planning.
"My doctor sat me down and said we should talk about what the next few years would look like. That's the conversation you don't want to have. That was fourteen months ago. I went home and my daughter had already ordered the IONShield — she'd been reading about it for weeks. I didn't have much hope. I'm going to tell you what I told my doctor at my last appointment: I'm not having that conversation anymore. My numbers stabilized. I'm walking my dog again. I'm sleeping through the night. Whatever we were going to discuss about the future — I think we can hold off."
Current status: Disease progression halted per physician assessment. Hospice planning discussion tabled indefinitely.
What The Nurses Are Seeing
The Ohio nurse who first tipped me off wasn't alone.
"I've started asking every patient whose numbers improve what's changed at home. More than half of them mention an air ionizer. I don't say anything officially because I can't. But personally? I have one in every room of my house."
— Pulmonary care nurse, Tennessee
"You can tell which homes have ionizers within ten minutes of walking in. The patients just look different. They're sitting up straighter. They're not reaching for the inhaler while we're talking. The air feels different too — I know that sounds unscientific but it's consistent."
— Home health nurse, Michigan
"I've recommended ionizers to patients off the record for three years. I can't put it in a care plan. But I can tell a patient's family member that there's interesting research on indoor ion concentration and let them draw their own conclusions. The ones who figure it out tend to come back looking better."
— Respiratory therapist, Florida
The Number That Stopped Me
Across the 23 patients I interviewed, I calculated the following:
Average reduction in rescue inhaler use: 71%
Average improvement in reported morning oxygen saturation: 2.1 points
Patients reporting zero exacerbations in the period following IONShield use: 17 of 23
Patients whose pulmonologist acknowledged measurable improvement in their clinical data: 19 of 23
Patients who said they would give up their IONShield before they'd give up any other single thing in their COPD management protocol: 23 of 23
Every single one.
My Verdict After Six Months Of Investigation
I've been a health journalist for eleven years. I've investigated pharmaceutical pricing, hospital billing fraud, supplement scams, and medical device failures. I am not easy to convince.
I am convinced.
What is happening with IONShield and COPD patients is not anecdotal noise. It is not placebo. It is not a coincidence distributed across 23 unconnected people in seven different states who never spoke to each other and arrived at the same outcome independently.
It is a pattern. A reproducible, measurable, clinically-acknowledged pattern that the standard COPD care model has no framework to explain — because it doesn't involve anything the standard COPD care model sells.
The science is real. The mechanism is established. The results are documented.
And the device costs thirty-nine dollars.
What I Would Do If I Had COPD
I want to step out of journalist mode for a moment and just be direct with you.
If I had COPD — if my FEV1 was declining, if I was reaching for a rescue inhaler before I finished my morning coffee, if I had been told to start thinking about supplemental oxygen — I would not wait.
I would not wait for my pulmonologist to recommend this. He won't. Not because it doesn't work. Because it sits outside every system he operates inside of. Because there's no billing code for "plug in the $39 device." Because the clinical guidelines move a decade behind the research and the research is sitting in journals he doesn't have time to read.
I would not wait for a clinical trial. The patients I spoke to did not wait for a clinical trial. They are breathing.
I would go to the IONShield website tonight. I would read the 11,000 reviews from people who bought it for allergies and sleep and ended up writing paragraphs about their lungs. I would order it. I would plug it in. And I would start tracking my morning oxygen saturation every day in a notebook, exactly the way Victor's wife did.
Because the downside of trying a $39 device is $39.
And the upside is what I watched happen to 23 people who were losing this fight and then stopped losing it.
What Happens When You Order
IONShield ships within 24 hours. It arrives in standard packaging, plugs into any standard outlet, and begins working immediately. There is no setup. There is no app. There is no filter to install or schedule to program.
You plug it in and it starts emitting 500 million negative ions per second into your room.
That's it.
Most of the patients I spoke with reported noticing something within the first week — mornings that felt slightly easier, nights that felt slightly less restless. By week three the pattern becomes undeniable. By month two, several described what I can only call a threshold moment — a morning where they realized they hadn't thought about their inhaler yet, and it was already 10am.
That moment, for a COPD patient who has organized their entire existence around managing the next breath, is not a small thing.
It is everything.

The 30-Day Guarantee
IONShield comes with a full 30-day money-back guarantee.
You don't pay to find out if this works for you. You try it for a month — the same month that most patients in my investigation started seeing measurable changes — and if your mornings don't feel different, if your inhaler use hasn't shifted, if you don't notice anything at all, you return it and pay nothing.
Thirty-nine dollars. Thirty days. Zero risk.
Against a disease that costs COPD patients an average of $4,800 per year and still lets it win.

30-Day Money Back Guarantee
Ships Within 24 Hours
Free Shipping Available
A Note On Availability
IONShield is not sold in retail stores. It is sold exclusively through their website, which means there are no distribution markups, no retailer fees — which is part of why the price is $39.99 instead of $150 for an equivalent device with a brand name on the box.
Current stock levels have been inconsistent. When my original draft of this investigation was shared in a COPD support group online, orders spiked and the device went briefly out of stock. I would not wait on this.
If you or someone you love has COPD — if you have watched a parent trade their independence for an oxygen concentrator, if you have stopped going to places because you can't trust your lungs to get you home, if you have had the conversation your doctor calls "planning for the future" and you know what that conversation really means —
This is worth thirty-nine dollars and thirty days of your time.
The patients I spoke with would tell you it was worth everything.
[GET IONSHIELD — OFFICIAL WEBSITE]
GET IONSHIELD NOW — LIMITED STOCK AVAILABLE[30-Day Money Back Guarantee | Ships Within 24 Hours | Free Shipping Available]
P.S.
After I filed this story, I received a message from the Ohio nurse who started all of this.
She told me her father — 74 years old, Stage 3 COPD, had been on her watch list for two years — had started using the IONShield three months ago on her quiet recommendation.
Last week he called her from his backyard.
He had walked out to check on his garden. By himself. Without stopping. Without oxygen. He wanted her to know that the tomatoes were coming in.
She said she hadn't heard him sound like that in four years.
"Like he had somewhere to be. Like he had time."
That's what clean air does.
Go get yours.
This is an advertisement and not an actual news article, blog, or consumer protection update. This website and the page that you are on may contain advertising content. The information provided in this article is for informational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Results described are not typical. Individual results may vary. These statements have not been evaluated by the Food and Drug Administration. Always consult your physician before beginning any new health protocol. © 2026 Health Dispatch. All rights reserved.