Podiatrist Who Treats Professional Athletes: “Nail Fungus From The Gym Won't Clear Because Everyone's Treating The Wrong Layer”

One Mistake. Fifteen Seconds. And It's Been Spreading Ever Since.
You know exactly when you got it. One day in the locker room, the pool deck, the communal shower — and you didn't have sandals on. Fifteen seconds you'd rather forget.
You probably figured it would clear up. Most guys do. You noticed the discoloration, made a mental note, got busy with other things. Checked it a few months later. Bigger than it was.
Maybe you grabbed something from the pharmacy — a cream, a spray, something that was supposed to handle it. You used it for a while. It didn't do much. Or it seemed to help and then came back.
So now it's been a year. Maybe longer. It's not affecting your performance. But it's there — spreading onto an adjacent nail, thickening up, starting to become a thing in a way it wasn't when it was still contained to one.
Before you try anything else, I need you to read this.
What I'm going to show you is the reason nail fungus from the gym doesn't respond to what you've tried — and it has nothing to do with the strength of the product or how consistent you were. It's a structural fact about your nail that every standard topical treatment is designed as if it doesn't exist.
Once you understand it, the failure rate of every cream in the pharmacy aisle will make complete sense.
More importantly: there's a method that accounts for that structural fact — and gets the antifungal compounds exactly where they need to go. Men who've had the same infection for one, two, even three years have cleared it in weeks using this. Not months. Not a prescription. Not a dermatologist's office.
It all comes down to one layer of your nail that standard topicals never cross.
I urge you to read this short article before you buy another product or book another appointment. What you're about to learn will change how you think about this problem — and make the right solution obvious.
The Sports Podiatrist Who Gave Athletes The Wrong Answer For 15 Years
My name is Dr. Marcus Hale. I'm a sports podiatrist based in Denver, Colorado — which means I spend my days looking at feet. Not ordinary feet. Feet that have run marathons, played five sets of tennis in 90-degree heat, trained twice a day for a college wrestling season, and worn the same athletic shoe for ten hours straight. Feet that have been subjected to every condition known to produce nail fungus.
I've been doing this for eighteen years. I've treated Division I athletes, masters marathon runners, military personnel returning from overseas deployments, and weekend warriors who train harder than most professionals. Nail infections are the most common non-injury foot complaint in every single one of those populations.
“Use this cream twice a day. Come back in six weeks if it doesn't clear.”
What I told patients for 15 years. It almost never worked.Here's what I told them for most of my career: "Use this cream twice a day. Come back in six weeks if it doesn't clear."
It almost never cleared.
I watched men cycle through the same three options — OTC cream, prescription oral antifungal, OTC cream again when they stopped the prescription — for years. They'd come back with the same infection, now on three nails instead of one. They'd tell me they'd been compliant. They were telling the truth. The failure wasn't their consistency.
The failure was mine — I was handing them tools that couldn't reach the problem.
It took me fifteen years and one specific conversation at a conference in Nashville to understand why. And once I understood it, I couldn't continue practicing the way I had been.
The Football Coach Who Made Me Question Everything I'd Been Telling Patients

Nothing prepared me for the day Jason Reed walked into my office.
Jason was 41 years old. High school football coach in Aurora, Colorado — spent thirty hours a week on practice fields and in locker rooms. He'd been coaching for twelve years. He knew the drill: shower sandals, dry your feet, keep your socks clean. He wasn't careless. He'd just had one afternoon where the post-game chaos meant he moved through the showers faster than he should have, without thinking about his feet.
That was eighteen months before he came to see me.
By the time he sat across from me, the infection had spread to four nails. His big toenail had thickened to almost double its normal height. The discoloration had crept from the nail edge across most of the nail bed. He wasn't in pain — not yet — but his cleats were starting to feel tight in a way they hadn't before.
"My wife brought it up last week," he said. Not angry. Just tired. "She was right. I've been putting this off too long."
He'd tried a pharmacy cream for two months when he first noticed it. Nothing. He'd looked into a prescription and decided against it when he read about the liver monitoring requirements — he was already managing a cardiac condition with medication and didn't want to add another drug to the stack. So he'd just been living with it.
I told him what I always told patients in his situation. Use this topical. Come back in six weeks.
He came back in six weeks. It was worse.
I handed him a different topical. Come back in six weeks.
He came back in six weeks. Still worse.
That was the night I stopped asking which treatment to try next — and started asking the question I should have asked fifteen years earlier:“Why isn't anything reaching this infection?”
Nashville. A Bar Graph. And A Number That Made The Entire Room Go Quiet.
Two weeks later I was in Nashville for the American Podiatric Medical Association symposium. It was the second afternoon of sessions — the kind of stretch where you've already been sitting in conference chairs for six hours and you're reading the schedule deciding if anything in the next block is worth staying for.
The last session of the day was listed as: "Topical Delivery Optimization in Nail Plate Pathologies: Penetration Rates Across Formulation Types." Dry title. I almost skipped it.
I didn't.
The presenter was Dr. Lena Vasquez, a pharmaceutical formulation chemist who'd spent the previous eight years studying how compounds travel through biological barriers — skin, nail plate, mucous membranes. She wasn't a podiatrist. She wasn't selling anything. She was presenting data.
She put a slide on the screen.
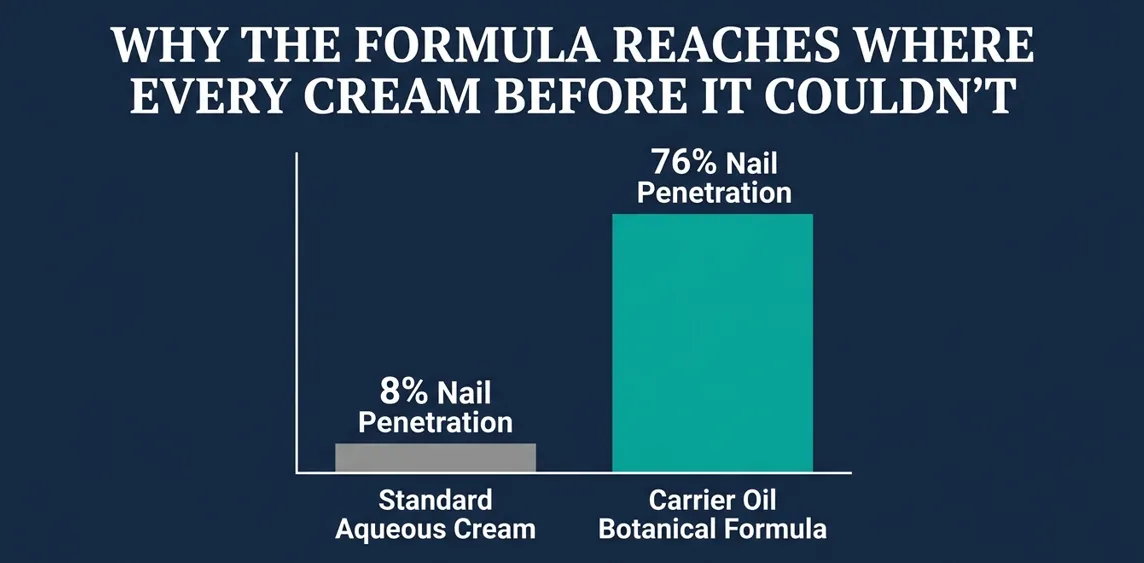
It was a simple bar graph. Penetration rates of various topical formulation types through the human nail plate, measured at 24 hours. The bars were devastating in their clarity:
Nail Plate Penetration Rates at 24 Hours
I wrote down 76% and underlined it twice.
Then she said something that made the room go quiet.
“The active ingredient in most topical antifungals works. It destroys fungal cell walls on contact. The question was never whether the molecule could kill the fungus. The question was whether the molecule couldreachit.”
— Dr. Lena Vasquez, Pharmaceutical Formulation Chemist"The active ingredient in most topical antifungals works. It destroys fungal cell walls on contact. The question was never whether the molecule could kill the fungus. The question was whether the molecule couldreachit. And in aqueous and alcohol-based delivery systems, the answer is almost always no."
She advanced to the next slide — a microscopy image I won't forget. She pointed to a layer of cells at the bottom of the frame.
"That's where the fungus lives. Right there. Below the nail plate. In eight years of testing standard topicals, I've never seen meaningful antifungal compound concentrations at that depth using conventional formulations."
She paused.
"But carrier-oil-delivered compounds are different. What I found is something nobody had thought to test."
I leaned forward in my seat.
What she explained next changed everything I thought I knew about treating this condition.
Why Every Cream You've Ever Used Was Aimed At The Wrong Target
Here's what Dr. Vasquez showed me — and what nobody has ever told you.
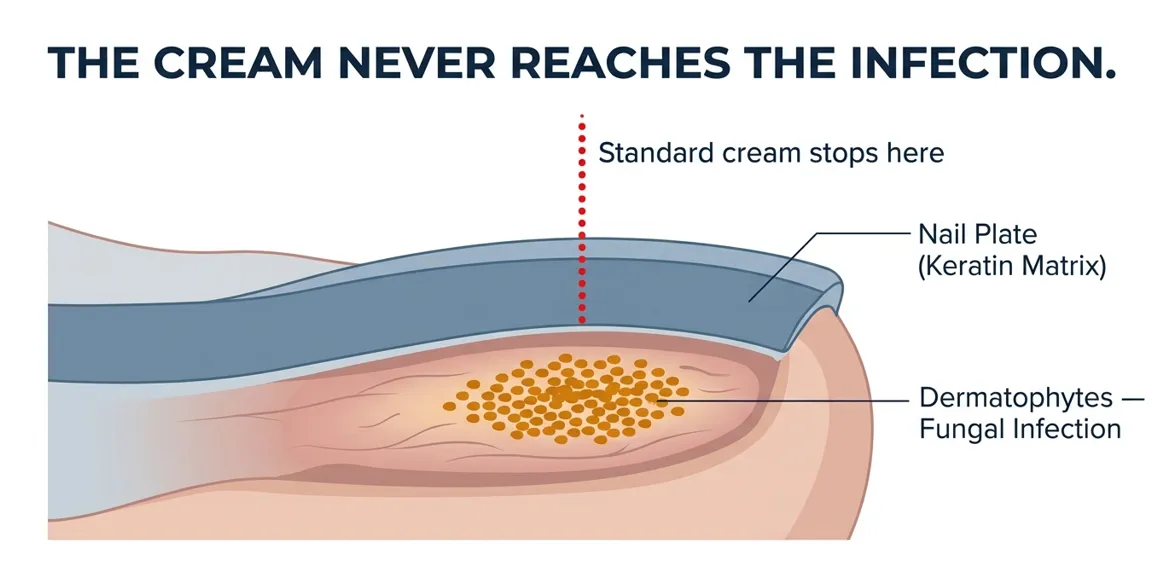
The nail plate — the hard surface you can see and touch — is not a window. It's a wall.
Specifically, it's a dense matrix of keratin proteins, layered and compressed in a structure designed to keep foreign substances out. It's the same mechanism that makes your nails hard instead of soft. It's a protective barrier that does its job extremely well.
Here's the problem: nail fungus doesn't live on top of the nail plate. It lives underneath it. The infection — dermatophytes, the family of fungi that feed on keratin — colonizes the nail bed, the soft tissue beneath the hard nail surface. That's where it reproduces. That's where it spreads. That's where the discoloration comes from, and the thickening, and the brittleness.
When you apply a standard cream or spray to an infected nail, here's exactly what happens: the product sits on the nail surface. The carrier — water or alcohol — evaporates within minutes. The active antifungal compound is left on top of a structure it has almost no ability to cross. The cream that "doesn't work" isn't weak. It's in the wrong place.
It's the equivalent of pouring water on your roof to fix a burst pipe in your basement.The solution is real. It's just aimed at entirely the wrong location.
This is why the clinical failure rate for standard OTC topical antifungals exceeds 60%. Not because the compounds don't work against fungi — they do. Because the compounds never reach the fungi.
It's why the cream you used for two months did nothing. It may have kept the nail surface clean. It did not reach the dermatophytes living 2-3mm below the nail surface.
It's why the infection kept spreading even when you were applying something twice a day. The infection was progressing in an environment with zero antifungal presence.
And here's what validates everything you've experienced: this is not a new problem. Dermatologists and podiatrists have known about the nail plate barrier for decades. It's documented in the literature. It's why oral antifungals — which bypass the nail plate entirely by traveling through the bloodstream — are so much more effective than topicals. The oral medication reaches the infection from beneath, through the nail bed's blood supply, instead of trying to cross the plate from above.
The problem with oral antifungals is a different issue, and I'll get to that next.
The point is this: nothing you've tried has worked because nothing you've tried was designed to cross the barrier. That is not your failure. It's a fundamental gap in the way topical treatments have been formulated for fifty years.
That gap is now closed.
The Four Known Ways To Cross The Nail Plate — And Why Most Men End Up At Option 4
Now that you understand why the infection hasn't responded, the question is simple: what actually gets antifungal compounds through the nail plate?
There are four known approaches. Three of them have serious limitations. The fourth is what I now recommend to every patient in Jason's situation.
Approach 1: Laser TreatmentLimited Access
Nd:YAG laser therapy works. The energy passes through the nail plate and heats the nail bed to a temperature that kills dermatophytes without damaging surrounding tissue. Clinical clearance rates run 60-80% depending on severity and number of sessions.
The problem is access and cost. A single session runs $500-1,000 at most clinics. Most infections require 3-4 sessions. You're looking at $1,500-3,000 minimum — cash pay, not covered by insurance. Most men don't do this. They should be able to. They can't.Approach 2: Prescription Oral AntifungalsLiver Risk
Terbinafine (Lamisil) and itraconazole are genuinely effective. They reach the infection through the bloodstream. Clearance rates for terbinafine run 70-80% for complete cure in controlled trials.
But the treatment course is 12 weeks of daily oral medication. Terbinafine carries documented hepatotoxicity risk — liver damage — requiring blood work before and during treatment. It interacts with a significant list of common medications. For a man managing any other health condition or on any other medication, it adds medical overhead that may be disproportionate to a nail infection. Many men read the prescribing information and decide against it. That's a reasonable decision.Approach 3: Prescription Topicals5–8% Cure Rate
Ciclopirox (Penlac) is the gold-standard prescription-strength topical antifungal. More concentrated than anything OTC. Dermatologists prescribe it regularly.
The problem should be obvious now: it's still a topical. It still faces the nail plate barrier. Complete cure rate in randomized trials: 5-8%. That's not a typo. The most prescribed topical antifungal for nail infections fails 90%+ of the time. Not because the compound doesn't work against fungi. Because delivery.Approach 4: High-Penetration Botanical DeliveryRecommended
This is the approach Dr. Vasquez's data pointed to — and it's the one nobody in conventional podiatry had been systematically using, because it came from outside pharmaceutical formulation entirely.
The principle: instead of water or alcohol as the carrier, use a base of penetrating oils — specifically oils whose molecular structure allows them to carry active compounds through keratin-rich tissue. These oils don't evaporate. They maintain extended contact with the nail surface. And they carry antifungal compounds through the nail plate in concentrations that aqueous and alcohol-based products cannot approach.
Pair that delivery system with a proven antifungal botanical — Tea Tree Oil, specifically terpinen-4-ol, which destroys fungal cell membranes on contact — and you have a topical that actually eliminates the infection.
This is the best approach for the overwhelming majority of men who aren't candidates for laser or don't want the prescription. Here's where it came from and exactly how it works.
Tea Tree Oil Has Killed Nail Fungus For A Century. The Problem Was Never The Ingredient.
Tea Tree Oil has been documented as an antifungal since the 1920s, when researchers began cataloguing the medicinal properties of Melaleuca alternifolia, the tree native to New South Wales. By the 1990s, controlled studies had established that its primary active compound — terpinen-4-ol — disrupts fungal cell membranes and causes the cell wall to collapse. It kills dermatophytes. That part was never in question.
The question, for a century, was how to get it where it needed to go.
What Dr. Vasquez had done — and what nobody in topical antifungal formulation had systematically attempted before — was test oil-based carrier systems for nail plate penetration. The insight was borrowed from cosmetic chemistry, where penetrating carrier oils had been studied for decades in the context of getting active compounds through skin barriers. She applied the same logic to the nail plate.
The result was the 76% penetration rate on that slide in Nashville.
But the delivery system isn't just about using oil instead of water. It's about which oils, in what ratios — and critically, how the formula maintains contact with the nail surface long enough to penetrate.
This is where the application format matters enormously.
A cream applied to a nail surface migrates within minutes. You rub it in, it spreads to surrounding skin, and the concentration at the nail surface drops. A spray lands and evaporates before meaningful penetration can occur.
A precision brush applicator — one that deposits the formula directly onto the nail in a controlled, even layer — changes the math entirely. The oils don't evaporate. They stay exactly where they're placed. Penetration happens over hours, not minutes, and antifungal compounds accumulate beneath the nail plate in concentrations that reach the dermatophytes and eliminate them.
The science was never missing. Tea Tree Oil's antifungal properties had been documented for a century. Carrier oil penetration through keratin had been established in cosmetic chemistry for decades. The gap was that nobody had put them together — properly calibrated formula, penetrating oil base, precision delivery format — and aimed the result at nail fungus.
That's the gap we closed.
14 Months. 12 Prototypes. The Formula That Finally Crosses The Barrier.
After Nashville, I came home and started working.
I knew what the formula needed to do: penetrate the nail plate, maintain sustained contact, deliver antifungal compounds in sufficient concentration to eliminate the infection. I knew the active compound — terpinen-4-ol from Tea Tree Oil. I knew the carrier system — a base of penetrating botanical oils rather than water or alcohol.
What I didn't know was how to build it precisely enough to work.
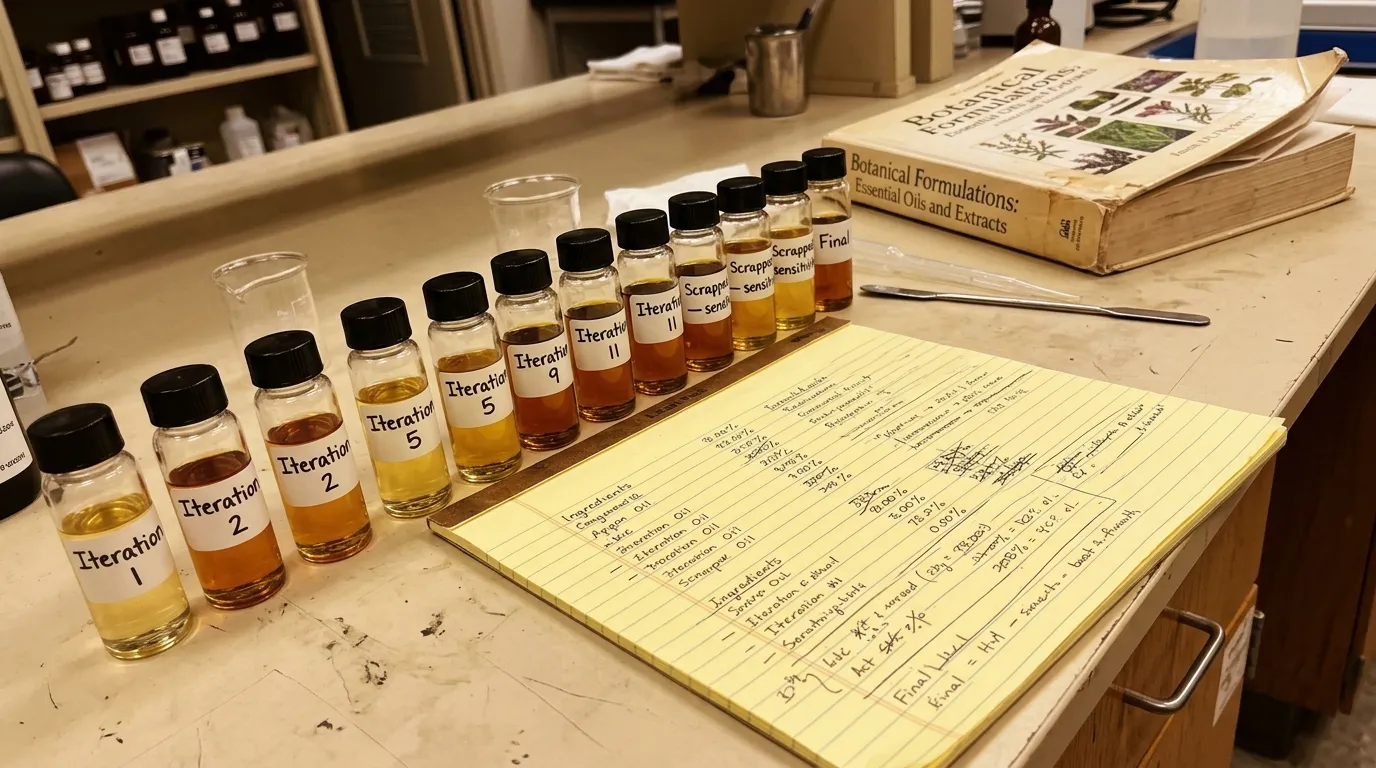
I spent the better part of a year in conversations with a botanical formulation lab in Portland. They'd been working in plant-based cosmetic chemistry for eleven years — the exact domain where carrier oil penetration had been studied most thoroughly. What I brought was eighteen years of clinical experience with the infection. What they brought was formulation science.
We went through twelve iterations. The penetration properties had to be right — get the carrier ratio wrong and the formula sits on the surface instead of crossing the plate. The consistency had to be right — too thick and it doesn't apply evenly; too thin and it migrates off the nail in minutes. The antifungal concentration had to be high enough to kill the infection but low enough to avoid irritating the surrounding nail bed tissue.
Three prototypes were scrapped entirely. Two showed the right penetration numbers in testing but produced skin sensitivity in wear trials. We reformulated twice.
Fourteen months after Nashville, we had a formula that worked.
Orivelle Formula — 17 Plant-Based Ingredients
Delivered via a precision pen applicator with a soft brush tip that deposits an even layer directly onto the nail surface. Twist the bottom to release the formula. Brush onto the infected nail and surrounding skin. No rinsing. No covering. Twice a day, under five minutes total.
We named it Orivelle.

The first person I gave it to was Jason Reed.
He'd been coming back to my office every six weeks for almost a year. Four nails, progressively worse. He'd tried three different products on my recommendation. None had worked. He was starting to seriously consider the oral antifungal despite his concerns about it.
I told him I wanted to try something different. I gave him the pen, showed him how to use it, and told him to come back in two weeks.
He came back in ten days.
"Something's happening," he said. He showed me his big toenail — the worst one, the one that had been thickened and discolored for over a year. The discoloration at the leading edge had started to fade. The surface was smoother than it had been. The infection wasn't gone. But it was visibly retreating for the first time in eighteen months.
"Keep going," I told him.
Six weeks after that, three of the four nails were completely clear. The fourth — the most advanced infection — was 70% clear and improving every week.
He wore open sandals to his daughter's pool party that summer. He texted me a picture of his feet.
I've been recommending Orivelle to patients ever since.
Real Men. Same Infection. Here's What Happened.



Orivelle is manufactured in small batches through a certified botanical processing facility. Each batch goes through quality control testing before it's cleared for shipment. We don't produce mass quantities and we don't keep large warehouse inventory.
Demand runs consistently higher than we plan for — men who clear their infection frequently order additional pens for family members, and for maintenance once the infection is gone. If you're reading this page, we likely still have units available.
That changes quickly. If the page is live, order now.
If you're thinking about grabbing a cheaper version online — don't.
What makes Orivelle work is the specific formulation: the carrier oil base, the ratios, the antifungal concentrations, and the delivery format. Generic antifungal pens on third-party marketplaces use aqueous or alcohol-base formulas — the same delivery system with the same 8-11% nail plate penetration that's been failing for decades. They're cheaper because they're not solving the problem. Orivelle is only available through our official website. That's how we control the formula quality.
What This Costs Everywhere Else — And What It Costs Here
Laser treatment at a clinic: $1,500-3,000. Multiple half-days off work.
A prescription terbinafine course: doctor visit, blood work, 12 weeks of daily medication, follow-up labs.
The topical treatments you've already tried: you know what those cost. You know what you got for it.
My initial recommendation to patients who can't do laser and don't want the prescription is a 3-pack of Orivelle — enough for a full treatment course across multiple affected nails. Through my clinic, patients pay $500 for a year's supply at wholesale.
That's not what Orivelle costs through this page.
Because we sell directly — no distributor, no clinic markup, no middleman — the price is a fraction of what you'd pay through a provider.
Claim Your Discount
Order Orivelle now — while this page is live and units are available.
CLAIM YOUR DISCOUNT — ORDER ORIVELLE NOWSecure checkout · Discreet packaging · Ships in 1-2 business days
Zero Risk. Thirty Days. No Questions.
You've spent money on this before and gotten nothing. That's exactly why I insisted on a 30-day money-back guarantee before I put my name on this.
You try Orivelle for up to 30 days. If you don't see visible improvement — if the discoloration isn't fading, if the infection isn't retreating — you contact our support team. Full refund. Not a partial credit. Not store credit. Your money, back.
No explanation required. No photos or documentation. No returning the product. You email us and the refund is processed, typically within 24 hours. Our support team responds within minutes, around the clock.
Your time, your money, and your results are completely protected. You are taking on zero risk by trying this.
Try Orivelle Risk-Free
30-Day Money-Back Guarantee · No Prescription Required · Nothing Entering Your Bloodstream
TRY ORIVELLE RISK-FREE — 30-DAY GUARANTEEFull refund within 24 hours if you don't see results · No questions asked
How To Order
- 1Click either button on this page.
- 2Select your package. If you have more than one affected nail, or want supply for a partner or family member with the same problem, the 3-pack is the right call. If you want maintenance supply after clearing the infection, the 6-pack gives you the best per-pen price.
- 3Enter your shipping and payment details. Orders ship in discreet packaging — nothing on the outside of the box indicates what's inside.
- 4Done. You'll receive a confirmation email with tracking. Most orders arrive within 3-5 business days.
Most men who've had this problem for more than a few months order the 3-pack. A single pen lasts 3-4 weeks with twice-daily use. If you have two or more nails affected, or if the infection is advanced, you want enough to complete the full course without stopping mid-treatment.
Order Now
Select your package and ship today.
ORDER NOW — SELECT YOUR PACKAGEFree shipping available · 3-5 business days delivery · Discreet packaging
The Alternative Is What You Already Know
Nail fungus doesn't stay where it is. These organisms feed on keratin. Your nails are keratin. Every adjacent nail is a potential next colony.
At one nail, this is manageable. At three or four, clearing it takes longer and requires treating a larger surface area. At the point where the infection is under multiple nails and in the skin between them simultaneously, you're looking at a multi-month protocol regardless of what you use.
Jason came to me at four nails after eighteen months of waiting. It took six weeks to clear three of them and another month for the fourth. If he'd found this when it was still on one nail, he would have been done in three weeks.
The men who sit across from me and say "I wish I'd tried something sooner" — that's the most common thing I hear. Not "I'm glad I waited." Not "it would have cleared on its own eventually."
Every week this sits untreated, the math gets slightly worse.
That's not going to be you. Not today.
This Is About More Than Your Nails
Nail fungus in active men is rarely just a cosmetic issue. It's the discomfort in your shoes that throws off your stride. It's the awareness at the pool, the beach, the locker room — the very place you picked it up. It's the quiet decision to keep your shoes on when you don't have to. It's the comment from a partner that you haven't been able to stop thinking about.
You've been managing this. Tolerating it. Mentally filing it under "deal with it someday."
Someday is a choice. So is today.
You know the infection isn't going to clear on its own. You know the pharmacy cream didn't work. You know the prescription comes with overhead you don't want.
Orivelle is the method that crosses the barrier those other options couldn't. Twice a day. Five minutes. Plant-based, nothing entering your bloodstream, no prescription required.
If it doesn't work for you — which based on 200,000 users and a 4.8-star average is unlikely — you get your money back. Every dollar.
Jason Reed wore sandals to his daughter's pool party after six weeks. Before that, he'd been avoiding showing his feet for eighteen months.
You've been dealing with this long enough.
Get Orivelle Now
Eliminate the infection at the source.
GET ORIVELLE NOW — ELIMINATE THE INFECTION200,000+ users · 4.8-star average · 30-day money-back guarantee