Dermatologist: Why Your Neighbor Cleared Her Nail Fungus And You're Still Dealing With Yours — The Answer Has Been Right Under The Nail This Entire Time
She had the same infection. She found one product. She cleared it in three weeks.
Here's the real reason her treatment worked when yours didn't — and how to clear the infection hiding beneath your nail plate in days, not months.

If someone close to you just cleared nail fungus that you've both been dealing with — you know the specific feeling that comes with that.
It isn't jealousy exactly.
It's something quieter and more frustrating: the same problem, the same starting point, a completely different outcome — and you don't know why.
You've probably told yourself her infection was milder. Or she got lucky. Or the timing happened to work out for her.
But some part of you suspects the real answer is simpler than that.
She found something that worked. You're still using something that doesn't.
And in a moment, I'm going to show you exactly why — because the answer comes down to one specific thing about how nail fungus works that nobody in a pharmacy ever explains.
It's not about how severe your infection is.
It's not about how long you've had it.
It's not about your immune system or your hygiene or how committed you are to the treatment.
It comes down to one barrier between the product you're using and the infection itself.
A barrier that every pharmacy cream, every spray, and every at-home remedy simply cannot cross — by design.
Once you understand this, you'll know exactly why her treatment worked and yours hasn't.
And more importantly, you'll know what to use instead.
I urge you to read this short article before you do anything else.
What I'm about to share is something I wish I'd told patients fifteen years earlier.
The Dermatologist Who Finally Understood Why Nothing Was Working

My name is Dr. Sarah Kimball.
I'm a board-certified dermatologist with 18 years of clinical practice. My patients have included professional athletes, Broadway performers, and executives who need to be in front of cameras and audiences — people for whom the appearance of their nails and skin is directly tied to their livelihood.
For the first decade of my career, I told every patient with nail fungus the same thing I was trained to tell them.
Try the pharmacy cream first. Give it eight weeks. If it doesn't work, come back and we'll talk about prescription medication.
I said it to hundreds of patients. I believed it was the right advice. I had no reason to doubt the protocol I'd been trained on.
What I didn't know — what nobody told me in medical school, and what I didn't learn until 2018 — is that the protocol I was sending patients home with had a documented failure rate above 60%.
Not because the ingredients don't work.
Because of where the infection actually lives — and where the cream doesn't reach.
When I finally understood what was happening, I felt something close to shame.
Not because I'd made an error. I'd been following standard of care.
But because I'd been watching patients cycle through the same treatments, get the same results, and come back more defeated each time.
And I'd had nothing new to offer them.
That changed when Carol walked into my office.

Carol W. was 54 years old when she first came to see me — a recently retired elementary school teacher from a suburb outside Columbus, Ohio.
She'd had toenail fungus for just over three years.
Two OTC cream courses. One full prescription round of terbinafine. And a brief experiment with tea tree oil she'd read about online.
The terbinafine had seemed to work — her nail cleared almost completely — and then six months after she finished the course, the infection was back. Exactly where it had started.
None of that was unusual. I saw it regularly.
What was unusual was why she'd made the appointment.
Carol paused.
I didn't have a good answer.
I ran through the standard script — her infection might be a more resistant strain, results vary between individuals, let's look at adding a prescription topical to her current regimen.
And Carol looked at me the way patients look at you when they know you're giving them the same answer that hasn't worked before.
I drove home that night thinking about her face.
I'd been practicing for 16 years. I had shelf after shelf of journals and clinical references.
And I couldn't tell a 54-year-old retired teacher why her coworker had cleared a longer, more entrenched infection in three weeks using something she bought online.
That was the night I stopped looking inside the standard dermatology protocol — and started looking outside of it.
What I Saw In Denver That Changed Everything
Two months after Carol's appointment, I attended the Annual Dermatology Research Summit in Denver.
Dr. Elena Voss — a nail and keratin structure specialist from the University of Utah — was presenting research on topical antifungal delivery and treatment failure rates.
The room was half full. Nail fungus isn't a glamorous conference topic.
But what she showed on her first slide stopped me.
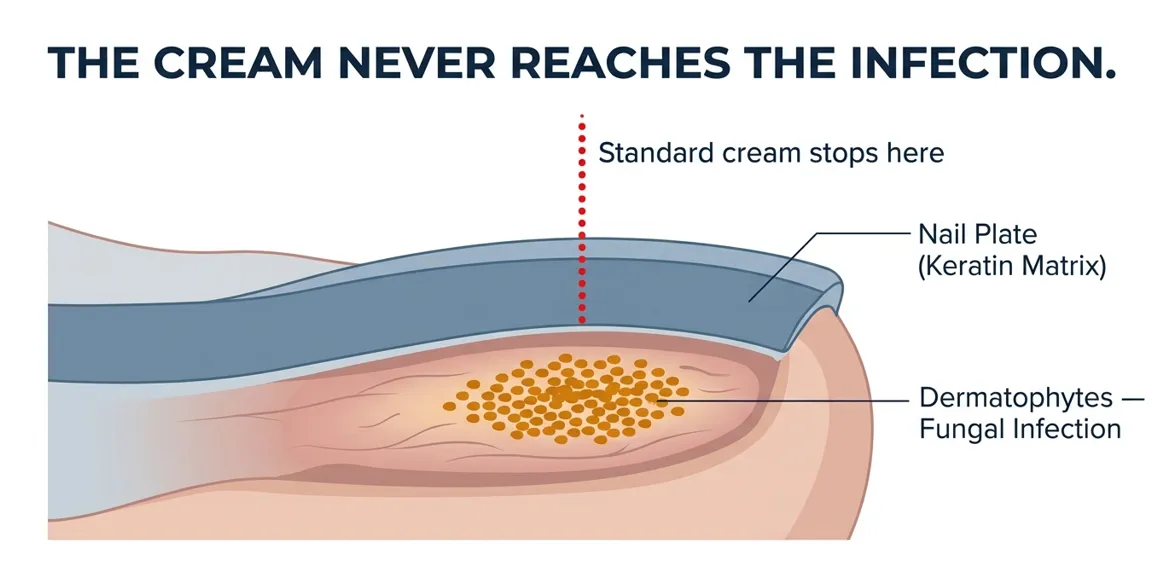
A cross-section of a toenail under high magnification.
She used a laser pointer to indicate two distinct zones: the nail plate — the hard, dense, compressed keratin structure visible on the surface — and the nail bed beneath it, where the soft tissue lives.
Then she put up a second image: the same cross-section, this time with blue dye tracing the path of a standard topical antifungal applied to the nail surface.
The blue stopped at the nail plate.
Not partway through. Not reduced in concentration.
It stopped completely. Pooled at the surface. Dispersed within minutes of contact.
Dr. Voss turned to the room.
She pointed to the nail bed in the image.
Below the barrier.
Untouched.
The room went quiet.
I thought about Carol.
I thought about 16 years of patients I'd sent home with products that had a 64% documented failure rate.
I wrote her name in the margin of my program.
What Dr. Voss showed on her third slide changed everything.
The Real Reason Her Treatment Worked And Yours Didn't
Here's what's actually happening when you have nail fungus and treatment isn't working.
The fungus — onychomycosis — doesn't live on top of your nail.
It lives under it.
Specifically, it lives in the nail bed: the soft keratin tissue beneath the nail plate. That's where it feeds, where it spreads, and where it has been growing since the day you first noticed the discoloration.
The nail plate — the hard structure you see and touch — is 25 to 30 compressed layers of dead keratin cells. Dense. Tight. Designed to protect the tissue underneath.
The problem is it doesn't distinguish between the fungus and the treatment.
A standard cream applied to the top of your nail disperses across the surface. Gravity pulls it toward the edges. Skin absorbs what runs off. Within minutes of application, the contact between the formula and the nail surface is broken — and whatever antifungal compound was in the cream has spread too thin to do anything useful.
Think of it this way: imagine your nail is a roof, and the leak is inside the wall.
The pharmacy cream is water poured on top of the roof.
It looks like it should be reaching the problem. But the wall is sealed. The water runs off. The leak continues.
That is not a metaphor. That is what is physically happening every time you use a cream and it doesn't work.
This is why your treatment seemed to improve the nail and then the infection returned — the surface improved while the infection underneath stayed active, waiting.
This is why terbinafine has a 10 to 50% recurrence rate — it reaches the infection via the bloodstream, but once you stop the oral medication, surviving spores in the nail bed reactivate.
This is why your coworker's nails look normal and yours don't.
She didn't have a milder infection. She didn't get lucky. She found a delivery method that crosses the nail plate.
You've been treating the roof. She found a way inside the wall.
The 4 Known Ways To Treat Nail Fungus (And Why #4 Is The Only One That Solves The Real Problem)
Now that you understand the penetration barrier, the question is simple: how do you get the treatment through it?
There are four known approaches. Here's what each one gets right — and where each one falls short.
Option 1: Oral prescription antifungals (terbinafine, itraconazole)
This bypasses the nail plate entirely by putting medication in your bloodstream instead. It reaches the infection. It works.
The trade-off: 12 weeks of daily oral dosing. Mandatory liver enzyme monitoring before you start and at 6 weeks — because terbinafine carries documented hepatotoxicity risk. Drug interactions with common heart medications, antidepressants, and blood thinners. A doctor visit, a prescription, lab work, and a willingness to monitor your liver function for a toenail infection.
Recurrence rate after stopping: 10 to 50%. The medication eliminates the visible infection but can't eliminate every dormant spore in the nail bed.
Option 2: Prescription topical lacquers (ciclopirox/Penlac)
The attempt to solve the penetration problem at the prescription level. Ciclopirox is formulated as a nail lacquer — the idea being that the lacquer creates a film that slowly releases antifungal compound into the nail.
Published cure rate: 29 to 36% after 48 weeks of daily application.
It's better than nothing. It doesn't solve the penetration problem.
Option 3: OTC pharmacy creams and sprays (Lotrimin, Lamisil AT, clotrimazole)
These products work on skin fungus — athlete's foot, ringworm, surface infections where the treatment reaches the pathogen directly. On nail tissue, with the barrier shown in Denver, they don't penetrate in therapeutic concentrations.
Published failure rate: exceeds 60% for most products in this category.
This is the option most people cycle through multiple times before giving up.
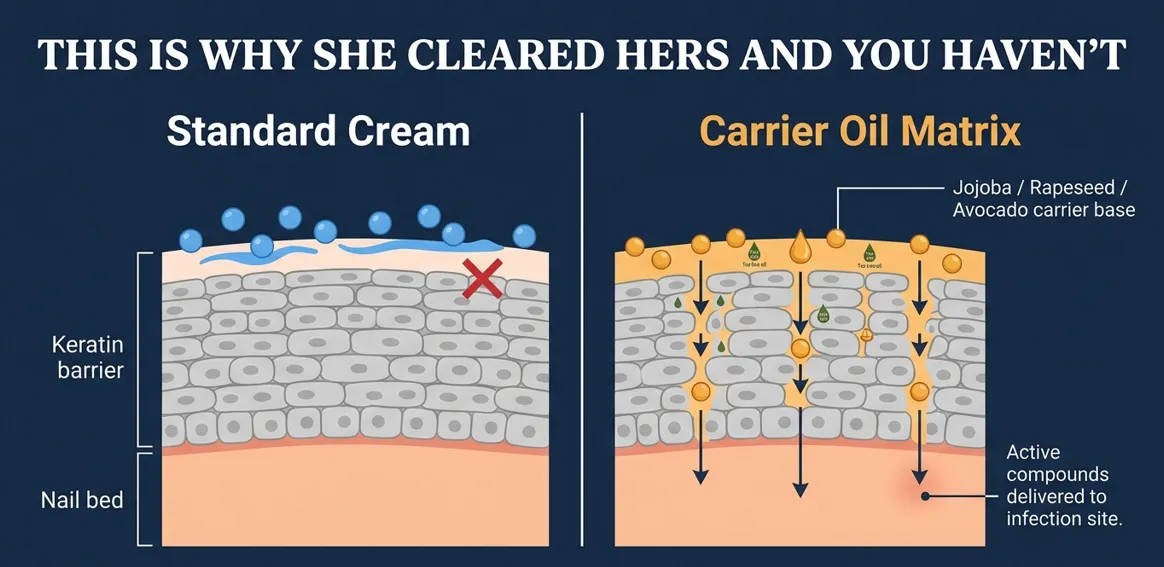
Option 4: Precision botanical delivery with a carrier oil penetration matrix
This is what Dr. Voss showed on her third slide in Denver.
Certain carrier oils — jojoba, rapeseed, avocado, camellia — have documented penetration characteristics through dense keratin tissue. Used in pharmaceutical transdermal delivery for this exact reason. Combined with concentrated botanical antifungals in a precision brush-application format that maintains sustained contact with the nail surface, the carrier oil matrix carries the active compounds through the nail plate where a cream dispersed across skin cannot.
The result: antifungal activity where the infection actually lives.
No prescription. Nothing entering your bloodstream. No liver monitoring.
This is why your neighbor's treatment worked. This is what she found online.

Why This Mechanism Actually Reaches The Infection
After Denver, I spent three weeks reviewing the research Dr. Voss had cited.
The carrier oil penetration concept wasn't new — it had been developed for wound care and dermal drug delivery, where getting an active compound through a skin or keratin barrier quickly is the entire point of the formulation.
What struck me was how obvious the application to nail fungus was — and how nobody in mainstream dermatology was talking about it.
I found research in theJournal of Pharmaceutical Sciencesquantifying the penetration of jojoba and rapeseed oil matrices through dense keratin tissue. At twice-daily application with sustained brush contact — meaning the formula was held against the nail surface rather than applied and immediately absorbed — the active compounds reached the sub-nail tissue within 72 hours of consistent use.
The mechanism isn't complicated. It's about contact time.
When you apply a cream, it disperses. Gravity pulls it. Skin absorbs the edges. The contact window between the formula and the nail surface lasts seconds.
A precision brush deposits a concentrated formula directly on the nail surface in a format that stays. The carrier oils don't run off — they penetrate slowly, carrying the botanical actives with them, maintaining the nail contact that makes delivery possible.
Combine that with tea tree oil — documented antifungal activity against Trichophyton rubrum, the most common species in nail onychomycosis, published in the Journal of Fungi— and 16 additional plant compounds, and you have a mechanism that reaches the infection and eliminates it.
The science was in the literature. The gap was in the delivery.
I called Carol two days later and told her I thought I'd found the answer to her question.
How I Made It Accessible
There was one problem.
The most effective clinical versions of this delivery system — the ones with documented penetration data — were professional treatments. Available through dermatologists and specialty nail clinics.
Cost: $800 to $3,000 per treatment course.
Carol was a retired teacher on a fixed income.
The majority of the patients I'd sent home with pharmacy creams for sixteen years weren't paying $3,000 for a toenail. They were going to Walgreens.
I'd found the mechanism that worked. I needed to make it accessible.
I spent four months working with a botanical formulation lab to develop a consumer version. The goal was a 17-ingredient formula combining the carrier oil penetration matrix — jojoba, rapeseed, avocado, camellia, evening primrose, and nine additional oils chosen for penetration and nail-conditioning properties — with a concentrated botanical antifungal complex built around tea tree oil, peppermint, and Lithospermum erythrorhizon, a plant compound with documented antimicrobial activity.
The delivery mechanism was the hard part.
The formula had to be thick enough to maintain sustained nail contact. Thin it too much and it runs off. Keep it too thick and the brush won't deposit it cleanly.
Fourteen prototype formulations. Too thin. Too thick. Too sticky. The brush tip absorbing the formula before it reached the nail.
Formulation 15 was right.
A twist-bottom pen that releases a precise dose to a soft-bristle brush tip with each turn. Brush it directly onto the nail surface and surrounding skin — no rubbing, no rinsing, no covering. The carrier oils maintain contact while the formula absorbs. Twice a day. Under five minutes.
I called Carol.
She came in the following Tuesday. I gave her three pens and told her to report back in three weeks.
Three weeks later she walked into my office without an appointment.
She sat down across from me and held out her foot.
Her nail looked clean. Not improved. Not partially cleared.
Clean.
The discoloration was gone. The thickening had stopped. The texture was normal.
She didn't say anything for a moment.
Then she said: "You should have found this a long time ago."
She was right. I should have.
That product is called Orivelle.
What Women Who've Used Orivelle Are Saying




A Note On Availability
Orivelle is manufactured in small batches.
The precision pen format — sealed brush tip, calibrated twist delivery, the carrier oil matrix that maintains viscosity stability through temperature changes — requires formulation and quality control that doesn't scale to mass production volumes.
Demand has grown significantly as more people find it through their networks. Orders regularly exceed our restocking cycle.
If you're reading this, we have units available today.
That can change.
Orivelle is available only through the official website. That's the only place you're getting the 17-ingredient carrier oil matrix formulated specifically to cross the nail plate.
What This Should Cost — And What It Actually Costs
A clinical nail treatment using the same penetration mechanism Orivelle is built on runs $800 to $3,000 per course through a specialist clinic.
Prescription terbinafine runs $50 to $300 for a full course — plus the doctor visit, plus the lab work, plus the monitoring appointments.
The average person with nail fungus spends between $400 and $1,200 on products before they find something that reaches the infection. Two pharmacy cream courses, a prescription cycle, maybe a dermatologist visit. And most of it was aimed at the surface of the nail.
When I priced Orivelle, my advisors told me $500 for a full treatment course was the right number.
I'm not in this for the margin. I'm in this because I watched a retired teacher tell me I should have found this a long time ago — and she was right.
Orivelle is listed at $59.99 per pen.
Today, for new customers, it's available at more than 60% off — $17.95 per pen.
That's less than a single copay at the dermatologist who told you to try the pharmacy cream first.
That's less than one tube of the Lotrimin that didn't work.
The three-pen pack — which covers a full treatment course for most infections — comes out to approximately $14 per penwith multi-pack pricing.
The six-pen pack, which gives you a complete treatment plus a maintenance supply, comes out to approximately $10 per pen— and you'll never run out mid-treatment.
| Package | Price Per Pen | Total | You Save |
|---|---|---|---|
| 1 Pen | $17.95 | $17.95 | $40 |
| 3 Pens (Best Seller) | $13.99 | $41.97 | $138 |
| 6 Pens (Best Value) | $9.99 | $59.94 | $300 |
Free shipping on all orders. Ships discreetly in standard packaging.
YES — CLEAR MY NAIL FUNGUS →You Take Zero Risk On This
Orivelle comes with a full 30-day trial period.
Use it every day for 30 days.
If your infection hasn't visibly retreated — discoloration lifting, flaking stopping, the nail starting to look normal — email our team atsupport@orivelle.com.
You'll get a complete refund. No questions asked. You don't have to send anything back.
Our support team responds within minutes, not days. 24 hours a day, 7 days a week.
You risk nothing. Either it works and you get your nails back — or you pay nothing.
There is no scenario in which you are out of money and still have nail fungus.
How To Order
- Click any button on this page
- Select your package — 1 pen, 3 pens, or 6 pens
- Enter your shipping details
- That's it
Most people order the 3-pen pack for a first course — enough formula to see clear, measurable results and enough supply that you won't run out mid-treatment.
If you have infection on more than one nail, the 6-pen pack gives you full coverage without reordering mid-treatment. A second nail, a maintenance supply, one for your partner — that's why most people who've done this before go straight to the six.
The discount pricing applies only while stock is available at current levels.
ORDER MY PACK NOW →Nail fungus doesn't stay the same.
It spreads.
It starts on one nail. Then the nail beside it. Then the nail beside that. Each infected nail is a reservoir the adjacent nail draws from — and it will, given enough time, humidity, and contact.
The longer you leave it, the larger your treatment need becomes. A one-nail infection that could have been cleared with one pen becomes a three-nail infection that takes months and multiple treatment courses.
And the social cost compounds too.
Every sandal season you skip. Every pedicure you sit out. Every time you pull your feet back when someone sits near you. Every summer you spend in closed shoes when you should be in flip-flops.
I've watched patients come in with a one-nail infection, leave it for 18 months, and come back with five infected nails.
Every single one of them said the same thing.
"I wish I had tried something sooner."
That's not going to be you. Not today.
Your neighbor didn't get lucky.
She found the one thing that actually reaches the infection — the thing every pharmacy cream and prescription cycle before it was aimed at the wrong side of the same barrier.
You've known something was off. You've known the treatments weren't reaching the problem. You just didn't have the language for it.
Now you do.
Orivelle is the precision botanical pen built to cross the nail plate and eliminate the infection where it lives. 17 plant-based ingredients. Twice a day. Under five minutes. Visible results in days.
This isn't about catching up to your neighbor.
This is about getting your nails back. Your feet back. Sandals in summer. Bare feet on your own floors. Pedicures without strategically placed polish.
You've been dealing with this long enough.
GET ORIVELLE — 60% OFF TODAY →Privacy Policy|Terms & Conditions|Contact Us|Refund Policy
© 2026 Orivelle. All rights reserved.
These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. Results may vary. The testimonials featured may have been shortened for clarity and are not necessarily representative of all users.